

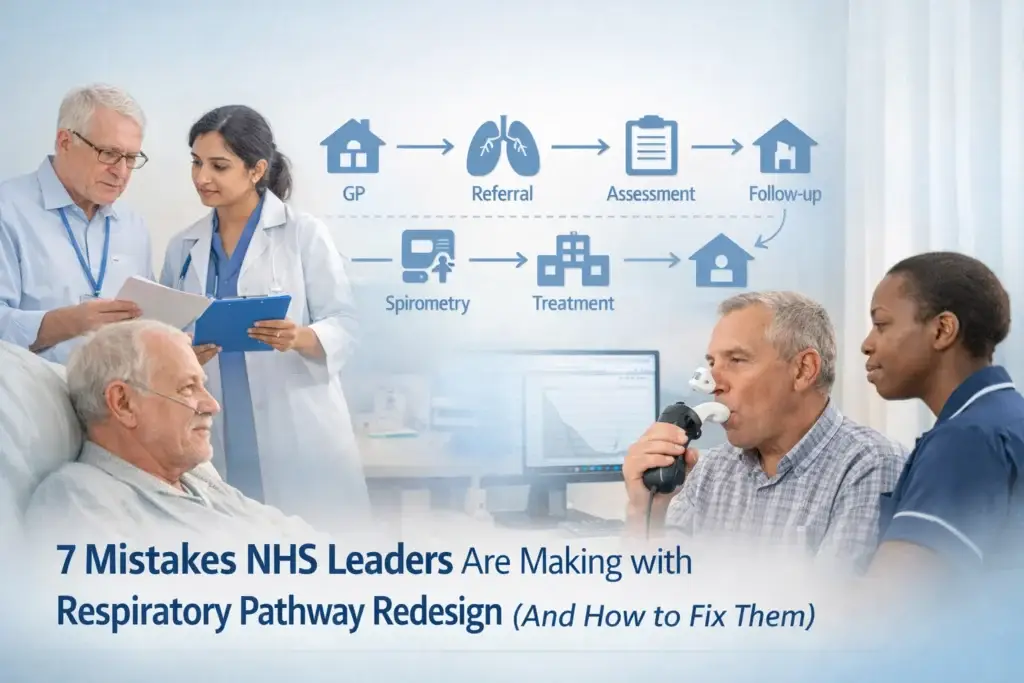
7 Mistakes NHS Leaders Are Making with Respiratory Pathway Redesign (And How to Fix Them)
category: NHS Strategy & Leadership
Respiratory services are being redesigned across England. That's not news. What's less discussed is how many Integrated Care Systems are repeating the same errors, often despite good intentions and genuine effort.
This isn't about blame. NHS leaders are working under extraordinary pressure, with limited resources and competing priorities. But when transformation projects are funded through initiatives like the Pathway Transformation Fund, getting the fundamentals right matters more than ever.
Here are seven mistakes we're seeing repeatedly, and what to do instead.
1. Treating Respiratory as a Single Service Line
The mistake: Planning for respiratory care as if it exists in isolation, separate from cardiology, mental health, social care and housing.
What this looks like on the ground: A respiratory lead designing a new pathway that improves spirometry access but doesn't connect to heart failure services, despite the fact that breathlessness often has multiple causes and patients rarely fit into neat diagnostic boxes.
The fix: Start with the patient journey, not the org chart. Map what actually happens when someone presents with breathlessness, from the GP surgery through diagnostics, across specialist input, and back into the community. Identify every hand-off point. Then ask: where does coordination fail? The NHS Long Term Plan explicitly calls for integrated care, but integration doesn't happen by accident. It requires clinical leads from different specialties sitting in the same room early in the design process.

2. Underestimating the Diagnostic Gap
The mistake: Assuming that diagnostic capacity, particularly spirometry, will somehow scale up through goodwill alone.
In practice, spirometry services were already stretched before the pandemic. COVID-19 significantly disrupted respiratory diagnostics, and many systems haven't recovered. Recent data shows that diagnostic backlogs persist, yet transformation plans often treat "improved access to spirometry" as a single line item rather than a complex workforce and infrastructure challenge.
The fix: Be specific. How many additional spirometry slots do you actually need per week? Who will deliver them, practice nurses, community respiratory teams, or a mix? What training, equipment and quality assurance is in place? The nine health systems recently awarded funding through the Pathway Transformation Fund are focusing heavily on diagnostic restoration for a reason. This isn't optional infrastructure. It's the foundation of everything else.
3. Ignoring the Social Determinants Sitting in Your Data
The mistake: Designing pathways that assume patients live in warm, dry homes with good air quality and reliable transport.
What patients and clinicians often describe: A perfectly designed care plan that falls apart because someone can't afford their heating, lives next to a busy road, or can't get to appointments without three buses.
The Marmot Review made this clear over a decade ago: health inequalities are driven by the conditions in which people are born, grow, live and work. Respiratory disease follows the same pattern. COPD prevalence is significantly higher in deprived areas, and asthma outcomes vary dramatically by postcode.
The fix: Build a respiratory pathway that explicitly addresses housing, air quality and fuel poverty. That might mean co-locating respiratory nurses with housing officers, or creating referral pathways into healthy homes schemes. It definitely means using your data to identify which neighbourhoods have the worst outcomes, and asking why. Then resource accordingly.

4. Letting Data Sit in Silos
The mistake: Designing transformation without tackling the fact that GPs, hospital teams, community services and social care still can't see each other's records in real time.
This isn't a technical observation. It's a lived reality for clinicians making decisions without full information, and for patients repeating their history at every appointment.
The fix: Make interoperability a non-negotiable part of your business case. Yes, it's complex. Yes, there are information governance hurdles. But every delayed discharge, every duplicated test, every missed medication change happens partly because systems don't talk to each other. NHS England's data strategy acknowledges this, but local systems need to push for practical solutions, shared care records, standardised coding, and clinical portals that actually work.
5. Designing Pathways Without Patients in the Room
The mistake: Treating "patient engagement" as a final-stage validation exercise rather than co-design from the start.
What this looks like: A finished pathway diagram presented to a patient group for feedback, when the fundamental assumptions have already been locked in.
People with lived experience of asthma, COPD or ILD know things clinicians don't. They know which parts of the pathway feel safe and which don't. They know where communication breaks down. They understand the difference between a service that works on paper and one that works in practice.
The fix: Involve patients before you draw the first process map. Not as a token gesture, but as equal partners in identifying problems and testing solutions. This takes time and requires proper support, expenses, accessible venues, plain English materials. But the alternative is designing services that look rational from a system perspective but don't reflect how people actually live.

6. Overlooking the Role of Community Pharmacy
The mistake: Designing respiratory pathways as if community pharmacy doesn't exist, or treating pharmacists purely as dispensers.
In practice, pharmacists are often the most accessible healthcare professional for people managing long-term conditions. They see patients frequently, they understand medication adherence, and they're trusted.
Recent policy shifts have expanded pharmacy's role in managing minor illness and supporting self-care, yet respiratory pathways rarely integrate pharmacy meaningfully. That's a missed opportunity, particularly for inhaler technique checks, medication reviews and identifying deterioration early.
The fix: Map where pharmacy sits in your respiratory pathway. Are pharmacists connected to respiratory nurses? Can they refer into pulmonary rehab or directly to specialists when needed? Do they have access to care plans? If the answer is no to any of these, you're leaving capacity unused.
7. Planning Without Workforce Reality
The mistake: Designing ambitious transformation projects without honestly assessing whether you have: or can recruit: the staff to deliver them.
Workforce is the constraint on almost everything in the NHS right now. Health Education England data shows persistent shortages across nursing, allied health professionals and GPs. Respiratory is no exception.
What this means: You can redesign a pathway, secure funding, and map every process: but if you don't have respiratory nurses, physiotherapists or consultants to staff it, nothing changes.
The fix: Start with workforce. How many whole-time equivalent staff do you need to deliver this pathway at scale? Where will they come from: redeployment, recruitment, or upskilling existing teams? What's the training pipeline? What about retention? Transformation that doesn't account for workforce reality isn't transformation. It's a document.

Moving Forward
None of these mistakes are unique to respiratory care, and none are easy to fix. But they're fixable: especially when clinical leaders, commissioners, Life Sciences partners and patients work together with clear sight of what's actually going wrong.
The nine systems currently testing transformation projects through the Pathway Transformation Fund have a chance to get this right and share what they learn. For everyone else, the lessons are already visible. The question is whether we're prepared to act on them.
If you're leading respiratory transformation in your ICS and want to connect with others doing the same work, join The Respiratory Network. We're creating space for the honest conversations that don't happen in formal meetings: including our upcoming Round Table 2026 event, where NHS leaders and Life Sciences partners come together to tackle exactly these kinds of challenges.
Because the stakes are too high to keep making the same mistakes.



Responses