

10 Reasons Your Respiratory Pathway Isn’t Meeting NRAP Standards (And How to Fix It)
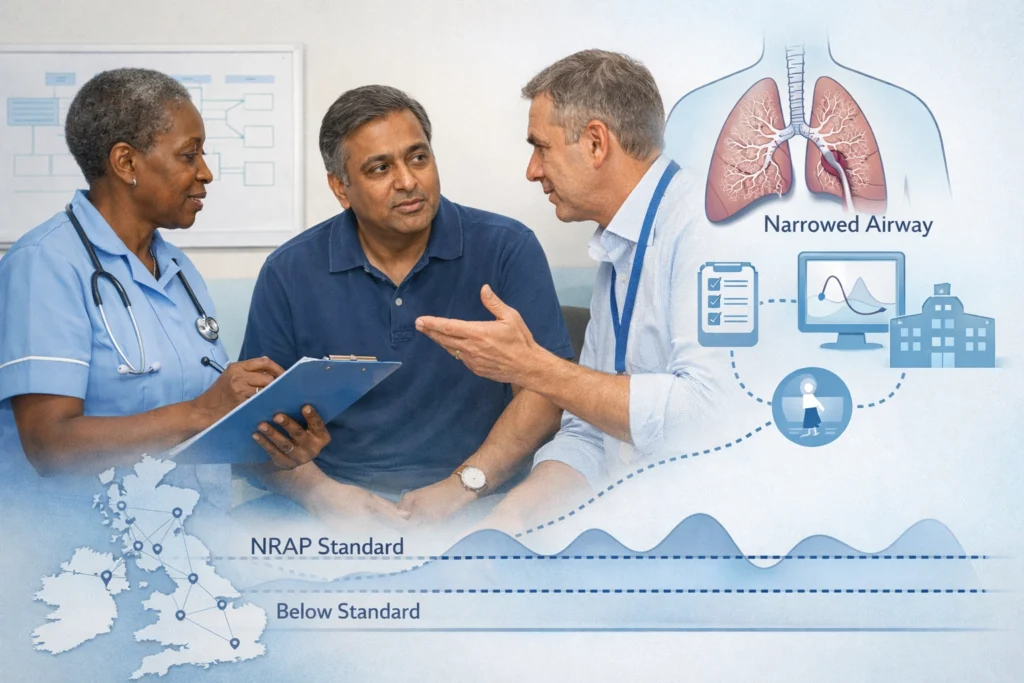
The National Respiratory Audit Programme (NRAP) serves as the primary compass for quality improvement within the UK’s respiratory landscape. For Integrated Care Boards (ICBs), clinical leads, and industry partners, these standards are more than just metrics; they are a reflection of how effectively a respiratory pathway serves the people relying on it.
However, the transition from audit data to clinical excellence is rarely a straight line. Many systems find themselves struggling to meet NRAP standards despite significant effort. Often, the barriers aren't found in a lack of clinical skill, but in the gaps between secondary care, primary care, and the patient’s lived experience.
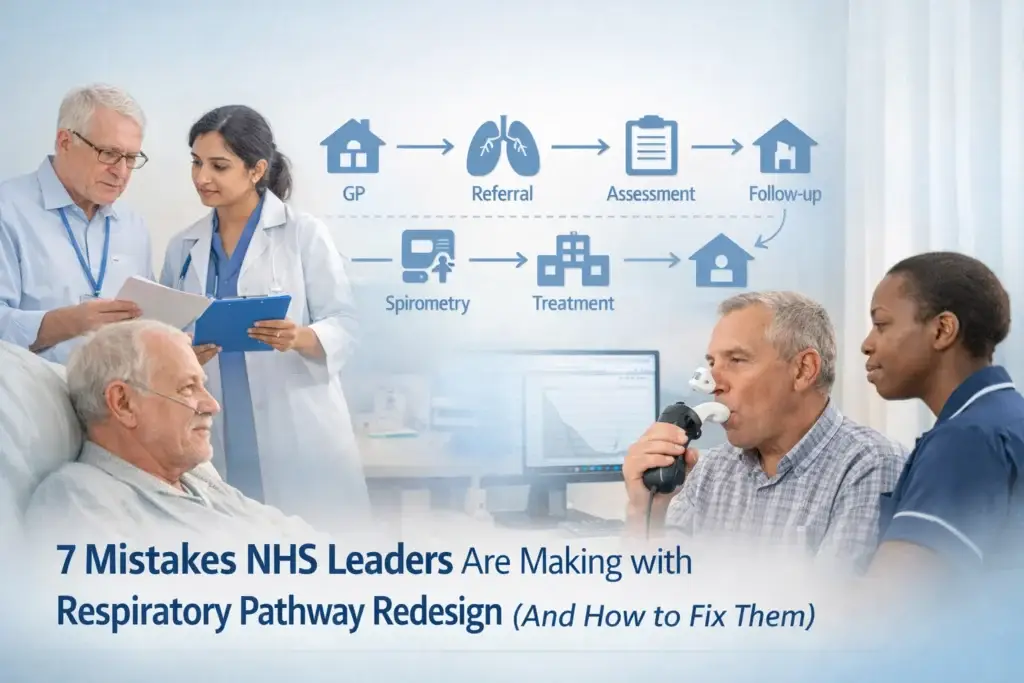
In practice, what we see on the ground is a system under immense pressure, where small administrative or procedural hurdles create significant bottlenecks. Below, we explore ten common reasons why pathways fall short of NRAP benchmarks and, crucially, how these can be addressed through collaborative action.
1. The Gap in Pulmonary Rehabilitation Enrollment
Pulmonary Rehabilitation (PR) is one of the most cost-effective interventions in the respiratory pathway, yet enrollment remains a major hurdle. Current data suggests only about 18% of people with stable COPD start PR within the 90-day referral window. This is a stark contrast to the 70% target set for May 2026.
The Fix: Improving these numbers requires a two-pronged approach. ICBs must ensure adequate resource allocation for PR services, but industry partners also play a vital role. By supporting the development of digital enrollment platforms or streamlined triage tools, the administrative burden on clinicians can be reduced, allowing for faster, more consistent referrals.
2. Inconsistent Participation in NRAP Audits
You cannot improve what you do not measure. A significant number of hospitals still struggle to meet the minimum case ascertainment target of 50%. Without a full data set, it is impossible to identify where a pathway is failing or succeeding.
The Fix: Success here is driven by leadership. Appointing dedicated NRAP clinical leads at the hospital level ensures that data collection becomes a built-in part of the workflow rather than an afterthought. When audit participation is viewed as a tool for local improvement rather than a top-down mandate, engagement naturally rises.
3. Variability in Discharge Bundles
The discharge bundle is the safety net that prevents readmission. Yet, for both COPD and asthma, the implementation of these bundles is highly variable. When a patient is discharged without a clear plan, the likelihood of a relapse increases significantly.
The Fix: Standardisation is the answer. Implementing digital or physical checklists that include every NRAP-required element: such as smoking cessation advice, inhaler technique review, and a personalised action plan: ensures that no patient falls through the cracks. Multidisciplinary oversight is essential to reinforce the completion of these bundles.

4. Delays in Acute Treatment for Children and Young People
Timing is everything in an emergency. NRAP standards highlight a concerning delay in the administration of systemic steroids for children and young people (CYP) with asthma, with fewer than half receiving treatment within the first hour of arrival.
The Fix: This is often a procedural issue. Introducing Patient Group Directions (PGD) in emergency departments allows nursing staff and appropriately trained clinicians to administer necessary treatments without waiting for a specific prescriber review. Removing these administrative steps can significantly improve the speed of care in the acute respiratory pathway.
5. The Documentation Deficit
What clinicians often describe is a "documentation burden" that takes them away from the bedside. However, poor documentation of medical assessments and treatment pathways leads to inconsistent care as patients move between different teams.
The Fix: Integrated care requires a shared language. Standardised asthma and COPD pathway booklets, accessible to all clinicians across the MDT, provide a clear roadmap. These booklets should include treatment guidelines and dosages to ensure every clinician, regardless of their specialism, is aligned with NRAP standards.
6. Overlooking Inhaler Technique Review
It is well-documented that many patients struggle with their inhaler technique, yet reviews are frequently missed during hospital stays or at discharge. If the delivery method for medication is ineffective, the medication itself cannot do its job.
The Fix: Inhaler technique review must be a non-negotiable component of every discharge assessment. This requires regular, brief training sessions for ward staff to ensure they are confident in verifying a patient's technique. Industry partners can assist here by providing educational resources and physical demonstration tools.
7. Inadequate Peak Flow Monitoring in Acute Care
For adults with asthma, peak flow recording is a vital metric for assessing the severity of an exacerbation. Despite this, only about 10% of patients have a peak flow recorded within the first hour of hospital arrival.
The Fix: Standardise acute assessment protocols so that peak flow measurement is treated with the same urgency as heart rate or blood pressure. Ensuring that equipment is readily available in all assessment areas and that staff are competent in recording and interpreting results is a fundamental step in meeting NRAP standards.

8. The Missed Opportunity for Tobacco Dependency Intervention
Smoking cessation is the single most effective intervention for long-term respiratory health. However, NRAP data shows that only about 40% of patients identified as current smokers have their tobacco dependency addressed during their hospital stay.
The Fix: Tobacco dependence intervention should be integrated into every discharge bundle. Rather than viewing it as an "extra" task, it must be seen as a core clinical requirement. Training staff to address dependency sensitively but effectively is key to shifting these numbers.
9. Delays in Specialist Respiratory Review
The target for a specialist review within 24 hours of admission is a cornerstone of NRAP for COPD patients. Achieving this requires a highly coordinated effort between the emergency department and the respiratory team.
The Fix: Clear referral pathways must be established to ensure that respiratory specialists have the capacity and the alerts needed to review admissions quickly. Strengthening the relationship between acute medicine and respiratory services helps ensure that specialist expertise is applied early in the patient journey.
10. Slow Access to Non-Invasive Ventilation (NIV)
For patients requiring NIV, delays can be critical. Currently, only about 60% of COPD patients receiving NIV get it within the two-hour window of arrival.
The Fix: Improving NIV access requires clear triggers for assessment and a well-trained workforce. Having dedicated NIV equipment and protocols in acute areas, rather than just on specialized wards, can reduce the time to treatment significantly.
The Role of Collaboration
Meeting NRAP standards is not a task that the NHS can achieve in isolation. The Respiratory Network believes that the most effective solutions come from the intersection of clinical expertise, patient lived experience, and Life Sciences insight.
When industry partners act as solution providers: helping to fix the "plumbing" of the pathway through data, education, and digital tools: the entire system benefits. For the clinician, this means more time for care. For the patient, it means a pathway that is safe, effective, and responsive.
Moving Forward
If your local respiratory pathway is struggling to meet these benchmarks, it may be time to look at the system-wide enablers. Are resources aligned with best practice? Is there a culture of data-driven improvement?
We invite you to join the conversation. Whether you are an NHS lead looking for best practices or a Life Sciences professional wanting to support pathway improvement, there is a place for you in our community.
- Join our community: Become a member of The Respiratory Network to access exclusive insights and networking.
- Attend our events: Join us for our upcoming Round Table 2026 to discuss these challenges in person.
- Follow us: Stay updated with the latest trends by following our social channels and visiting our main site.
Medical Disclaimer:
The content provided by The Respiratory Network is for informational purposes only. It is not intended to be a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. Never disregard professional medical advice or delay in seeking it because of something you have read on this website.




Responses