

Palliative Care in End-Stage COPD: Navigating the Reality of Lungs ‘Shutting Down’
End-stage Chronic Obstructive Pulmonary Disease (COPD) is a clinical reality that carries significant weight for patients, their families, and the healthcare professionals managing their care. In the UK, respiratory health is a major focus for NHS services, particularly as we look toward more integrated, community-based care models. However, the transition into the advanced stages of the disease: often referred to as Stage 4 or very severe COPD: remains a period of high anxiety and clinical complexity.
The phrase “lungs shutting down” is one often searched for by those seeking to understand the final progression of this condition. While the terminology is visceral, it reflects a genuine need for clarity on what the final stages of COPD look like and how palliative care serves to manage these symptoms. This blog explores the clinical landscape of advanced copd care uk, the symptoms of disease progression, and the role of multidisciplinary support in ensuring dignity and comfort.
Understanding the Progression to End-Stage COPD
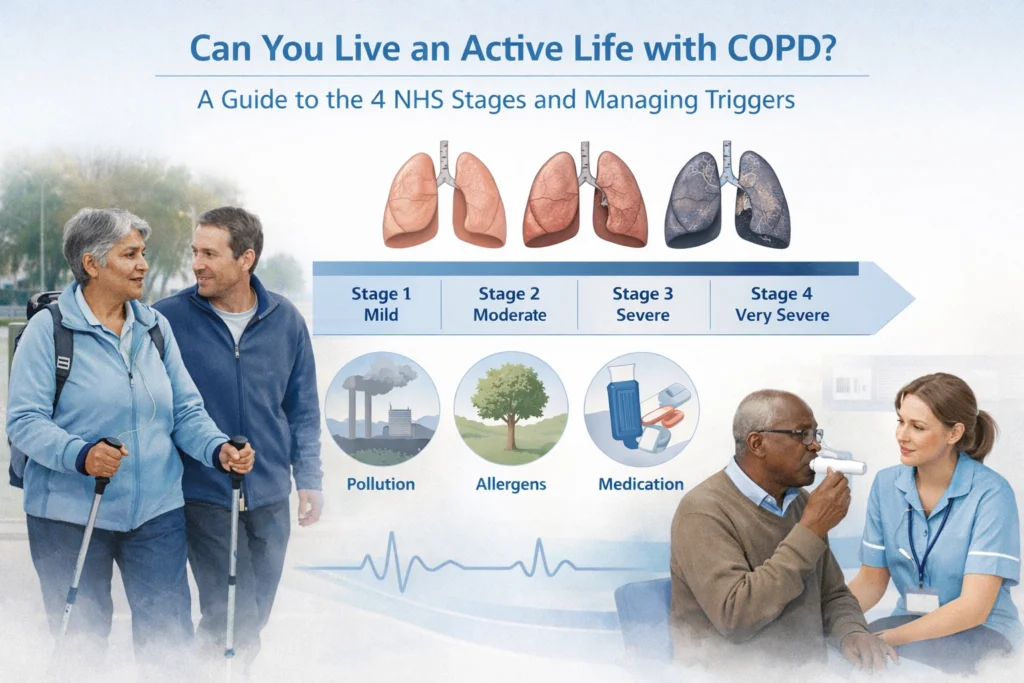
COPD is a progressive condition characterized by airflow obstruction that is not fully reversible. In the UK, the National Institute for Health and Care Excellence (NICE) and the Global Initiative for Chronic Obstructive Lung Disease (GOLD) provide the framework for staging this progression. By the time a patient reaches the “end-stage,” they typically experience severe breathlessness (dyspnea) even at rest, frequent exacerbations, and a significant decline in their quality of life.
In practice, clinicians often observe a “flicker” effect in late-stage COPD: periods of relative stability punctuated by sudden, severe declines. Unlike some other terminal conditions where the trajectory is a steady decline, COPD progression can be unpredictable. This makes the early integration of palliative care essential within NHS respiratory services.

What Does Palliative Care Look Like for End-Stage COPD?
There is a common misconception that palliative care is synonymous with hospice or the final days of life. In reality, palliative care for respiratory patients focuses on symptom management and quality of life, and it can be introduced alongside active treatments.
For someone with advanced COPD, palliative care involves a coordinated effort between GPs, respiratory consultants, community nurses, and social care. The primary goals are:
- Symptom Relief: Addressing refractory breathlessness, cough, and fatigue.
- Psychological Support: Managing the high levels of anxiety and depression that often accompany the feeling of being unable to breathe.
- Advance Care Planning (ACP): Documenting the patient’s wishes regarding hospital admissions, non-invasive ventilation, and resuscitation.
Clinical papers, such as those published in the European Respiratory Review, emphasize that early palliative intervention reduces the number of crisis-led hospital admissions and improves patient satisfaction (Higginson et al., 2014). This approach is a cornerstone of pathway excellence, ensuring that the patient remains at the centre of the decision-making process.
The Reality of ‘Lungs Shutting Down’: Symptoms and Signs
When people ask what it feels like when lungs are “shutting down” in the context of COPD, they are often describing the physiological transition where the respiratory system can no longer maintain adequate gas exchange. This is known as respiratory failure.
In the final stages, several key symptoms become more prominent:
- Increased Respiratory Effort: The use of accessory muscles (in the neck and shoulders) to breathe becomes constant.
- Hypercapnia (Carbon Dioxide Retention): As the lungs struggle to exhale CO2, patients may become increasingly drowsy, confused, or experience persistent headaches.
- Cyanosis: A bluish tint to the lips, fingernails, or skin, indicating low oxygen levels in the blood.
- Refractory Dyspnea: Shortness of breath that no longer responds to standard inhaled therapies or supplemental oxygen.
- Changes in Breathing Patterns: In the very final stages, breathing may become irregular or shallow.
It is important to note that while these signs are distressing to witness, the goal of palliative care is to manage these sensations. Through the use of various pharmacological interventions (excluding specific drug names here) and non-pharmacological techniques like fan therapy or positioning, the sensation of “air hunger” can be significantly diminished.
Navigating the Final Stages Before Death
The final stages of COPD are often characterized by a decrease in physical activity and an increase in time spent sleeping or resting. Patients may lose interest in food and drink, which is a natural part of the body slowing down.
Clinically, the focus shifts entirely to comfort. This often involves moving the patient to their preferred place of care: whether that is at home, in a hospice, or within a dedicated hospital ward. In the UK, the focus of respiratory health uk is increasingly on facilitating home-based palliative care, supported by community respiratory teams who understand the specific nuances of COPD.
What the end looks like for someone with COPD depends heavily on the support systems in place. With a robust advance care plan, the transition can be managed without the trauma of unnecessary emergency interventions. This is a topic we frequently discuss in our public forum, where both clinicians and those with lived experience share insights on navigating these difficult conversations.
The Importance of Advance Care Planning
One of the greatest challenges in COPD care is the timing of end-of-life discussions. Research suggests that these conversations often happen too late, or not at all, due to the unpredictable nature of the disease.
Advance Care Planning (ACP) is not just a legal document; it is a clinical process. It allows the patient to voice what matters most to them. Does the patient want to avoid the ICU? Is being at home more important than life-prolonging measures? Within the framework of NHS strategy leadership, there is a strong push to make these discussions a standard part of the respiratory pathway.
For the Life Sciences sector, understanding this stage of the patient journey is vital. Innovation isn’t just about new therapies; it’s about better delivery systems and monitoring tools that help keep patients comfortable and stable in their preferred environment for as long as possible. You can explore more on this in our Life Sciences Innovation category.
“Before we proceed, a note from our colleague Linda: The information provided in this blog is for educational and informational purposes only and does not constitute medical or legal advice. Always seek the advice of a qualified healthcare professional regarding any medical condition.”
Collaborating for Better End-of-Life Care
At The Respiratory Network, we believe that improving the end-of-life experience for COPD patients requires a unified approach. Clinicians need the resources to hold these difficult conversations, patients need the platform to share their lived experiences, and industry partners need to align their goals with the reality of the NHS frontline.
Managing end-stage COPD is one of the most demanding aspects of respiratory medicine. It requires a blend of clinical expertise, deep empathy, and a commitment to dignity. By addressing the “burning questions” surrounding the final stages of the disease, we can strip away some of the fear and replace it with a structured, compassionate plan.
Join the Conversation
The transition to palliative care in respiratory health is a complex journey, but you don’t have to navigate it alone. Whether you are a clinician looking for pathway excellence, a patient advocate, or a Life Sciences professional, your voice is essential to improving the system.
- Become a Member: Join a community dedicated to respiratory health. Sign up here.
- Attend Our Next Event: Be part of the conversation at the The Respiratory Network Round Table 2026.
- Follow Us: Stay updated with the latest clinical updates and data insights on our social media channels.
Together, we can ensure that every stage of the respiratory journey: including the very last: is met with the highest standard of care and understanding.
References for Further Reading:
- NICE Guideline [NG115]: Chronic obstructive pulmonary disease in over 16s: diagnosis and management.
- British Thoracic Society (BTS) Guideline for Pulmonary Rehabilitation in Adults.
- Higginson, I. J., et al. (2014). An integrated palliative and respiratory care service for patients with advanced disease and refractory breathlessness: a randomised controlled trial. The Lancet Respiratory Medicine.
- Cochrane Review: Interventions for managing breathlessness in patients with advanced disease.


Responses