

Why the 'Postcode Lottery' is Still the Biggest Challenge in UK Respiratory Care

If you live in the wrong part of England, your chances of being admitted to hospital with an asthma attack can be five times higher than someone in another region. For COPD, the variation is equally stark. This isn't news to anyone working in respiratory care, but it remains one of the most stubborn problems the NHS faces.
The 'postcode lottery' is shorthand for a complex web of structural inequalities. It's not about one trust being better than another. It's about funding formulae, workforce distribution, commissioning priorities, and decades of investment decisions that compound over time. And for patients with chronic respiratory conditions, the consequences are measured in hospital admissions, lung function decline, and years lost.
What the Postcode Lottery Looks Like on the Ground
In practice, it shows up in ways that are both obvious and subtle.
One ICB might have a well-resourced respiratory service with dedicated community teams, virtual wards, and timely access to pulmonary rehabilitation. Another, 30 miles away, might be managing with a skeletal service where patients wait months for follow-up and spirometry is rationed. The clinical need doesn't differ. The response does.

The National Asthma and COPD Audit Programme has consistently highlighted variation in care quality across England and Wales. Emergency admissions for asthma and COPD vary wildly between regions, even after adjusting for population health and deprivation. Some areas have admission rates that are double the national average, while others sit well below it.
This isn't just about acute care. Access to specialist respiratory services, diagnostic tools like FeNO testing, and biologics for severe asthma all follow similar patterns. If you're diagnosed in one part of the country, your treatment pathway might look entirely different to someone with the same condition elsewhere.
Patients and clinicians both describe the frustration of knowing what good care looks like, but not being able to access it consistently.
Why It Persists
The reasons are rarely simple, and they don't fit neatly into a single explanation.
Funding allocation is part of it. The NHS uses a weighted capitation formula to distribute resources, but it doesn't always reflect the true burden of respiratory disease in an area. Regions with older populations, higher smoking rates, and greater air pollution often need more respiratory resource, but they don't always get it. Historical investment patterns also matter. Areas that invested heavily in respiratory infrastructure 15 years ago still benefit today. Those that didn't are playing catch-up with fewer resources.
Workforce is another factor. Respiratory specialist nurses, physiotherapists, and consultants are not evenly distributed. Some trusts have built strong multidisciplinary teams. Others struggle to recruit and retain, particularly in more rural or deprived areas. The result is that expertise clusters in certain places, while others rely on generalists managing complex respiratory caseloads alongside everything else.
Commissioning priorities vary. Integrated Care Boards have autonomy over how they spend their budgets, and respiratory doesn't always rise to the top. Cancer, mental health, and urgent care often command greater attention, particularly when national targets and political focus sit elsewhere. Respiratory care can become the thing that gets addressed when everything else is stable : which, in the current NHS, means it rarely gets addressed at all.
Then there's the question of system design. In some areas, respiratory care is well integrated between primary, community, and secondary care. Patients move smoothly through pathways, with clear escalation routes and shared decision-making. In others, services are fragmented. GPs refer into secondary care and then lose sight of the patient. Community respiratory teams exist but aren't connected to hospital discharge processes. Pulmonary rehab is commissioned separately and has a six-month wait. None of this is anyone's fault, but it compounds over time into something that looks a lot like a postcode lottery.
What Patients and Clinicians Experience
For patients, this variation can feel invisible until it isn't.
You might live in an area where your GP practice has a specialist respiratory nurse who runs regular asthma clinics, checks your inhaler technique, and adjusts your treatment proactively. Or you might be in a practice where respiratory care is done in 10-minute appointments by whoever is available, and your inhaler prescription is renewed without a review because there's no capacity to do anything else.
When exacerbations happen, the difference becomes more pronounced. Some patients are picked up by community respiratory teams within 24 hours of hospital discharge, with daily virtual monitoring and rapid access to treatment at home. Others are discharged with a follow-up letter to their GP and little else. The outcome data reflects this. Hospital readmission rates for COPD vary significantly between trusts, and much of that variation is avoidable.

Clinicians, particularly in under-resourced areas, describe working in a system where they know what patients need but don't have the tools to provide it. That might mean rationing spirometry, delaying referrals, or managing severe asthma without access to biologics because the local formulary doesn't include them. It's not about clinical skill. It's about infrastructure, funding, and the conditions in which care is delivered.
What Can Be Done
Fixing the postcode lottery isn't a single-solution problem, but there are levers that can reduce variation and improve equity.
National standards with local flexibility matter. The work that organisations like the British Thoracic Society and NHS England have done to define best practice in respiratory care provides a baseline. But standards only work if there's accountability for delivering them, and if ICBs are supported to implement them in ways that make sense locally.
Workforce planning needs to be more strategic. Respiratory specialist nurses and allied health professionals are the backbone of good community respiratory care, but they're in short supply. Training pipelines, retention strategies, and career pathways all need attention. Some trusts have solved this through innovative roles and skill-mix, but that learning doesn't always travel.
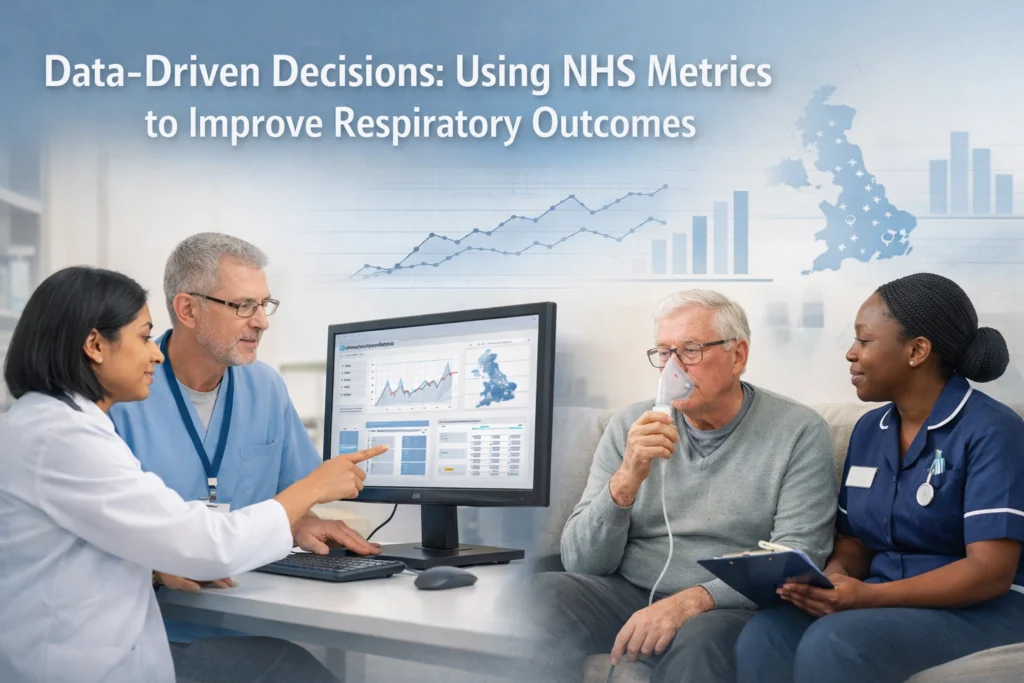
Better use of data and benchmarking can help too. When trusts and ICBs can see where they sit compared to peers, it creates constructive pressure to improve. The NACAP audits are valuable for this, but the data needs to be accessible, timely, and linked to quality improvement support.

Life Sciences has a role, but it's not about selling more products into the system. It's about working alongside NHS leaders to design services and pathways that work in practice, not just in theory. That might mean supporting implementation of remote monitoring, co-designing patient support programmes, or helping to build the evidence base for new models of care. The best partnerships are the ones where Life Sciences understands the constraints clinicians are working within and adapts accordingly.
Finally, patient voice needs to be part of the solution. People living with asthma and COPD know what good care looks like because they experience its absence. Involving patients in service design, pathway development, and quality improvement isn't a token gesture. It's how you build services that actually meet need.
What This Means for the Respiratory Community
The postcode lottery won't be solved by a single policy announcement or funding boost. It's structural, historical, and deeply embedded in how the NHS operates. But that doesn't mean it's inevitable.
What's needed is sustained attention, collaboration between NHS leaders and Life Sciences, and a shared commitment to reducing variation. That means being honest about where disparities exist, understanding why they persist, and working together to design solutions that are deliverable, not aspirational.
If you're working in respiratory care : whether as a clinician, a commissioner, or in Life Sciences : this is something you already know. The question is how we move from knowing about it to doing something about it.
Want to be part of the conversation? The Respiratory Network brings together NHS leaders, clinicians, patients, and Life Sciences to tackle challenges like this. Join us as a member or come along to our next Round Table event to shape the future of respiratory care together.


Responses