

Stop Guessing: Why Symptom-Based Assumptions are Failing the UK Respiratory Pathway
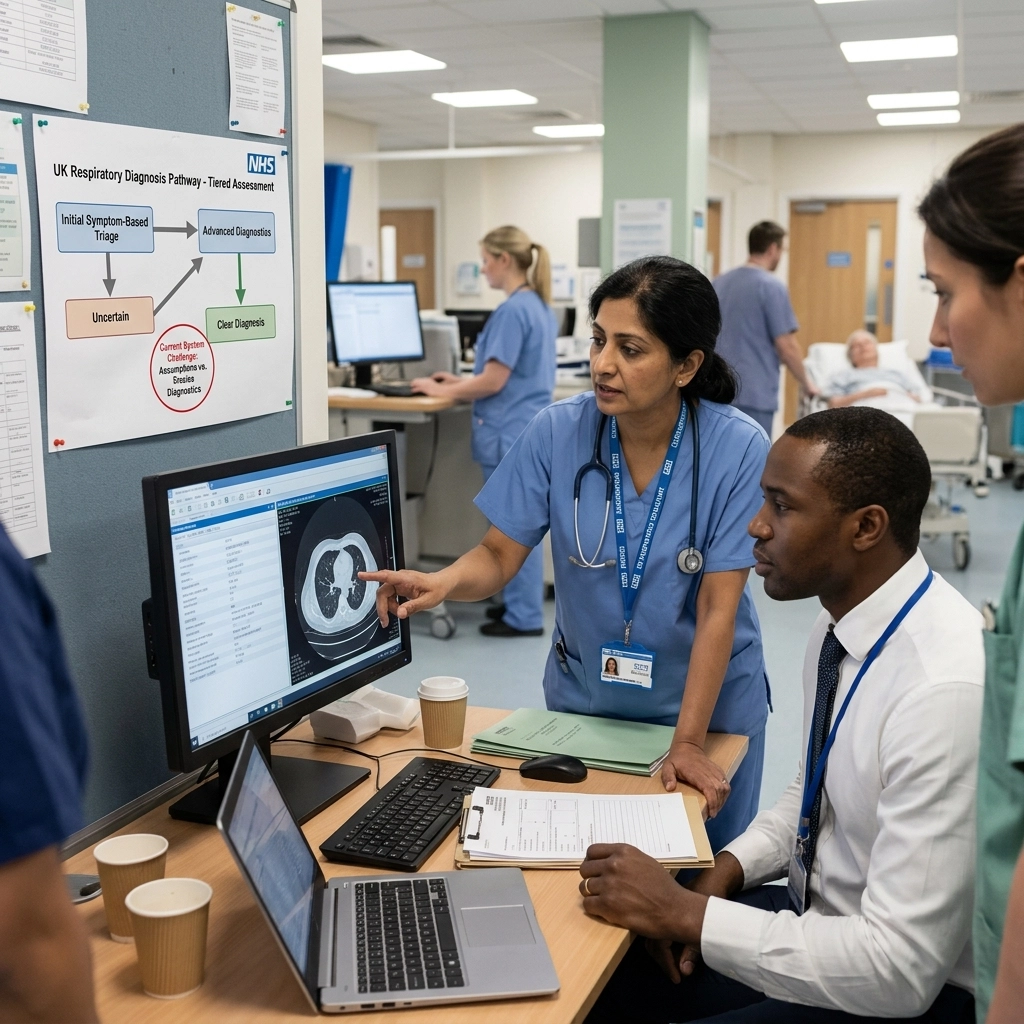
In the world of respiratory care, there is a phrase we hear often: "It’s probably just a touch of asthma," or "At your age, a bit of breathlessness is to be expected." While these assumptions are usually made with the best intentions, often in a time-pressured primary care setting, they are becoming a significant barrier to effective care.
For too many patients in the UK, the journey through the respiratory pathway begins not with an objective test, but with a guess. And in 2026, as our healthcare system grapples with backlogs and shifting demographics, "guessing" is a luxury we can no longer afford.
When we rely on symptom-based assumptions rather than objective diagnostics, we aren't just delaying a label; we are delaying the right treatment, increasing the risk of exacerbations, and ultimately placing a higher burden on NHS respiratory services.
The High Price of "Probably"
The most common diagnostic crossover we see is between Asthma and COPD. On paper, the symptoms can look remarkably similar: cough, wheeze, and shortness of breath. In practice, however, the underlying pathology and the required management are worlds apart.
Data frequently shows that a significant percentage of patients labeled with COPD actually have Asthma, and vice versa. Worse still, many patients are living with "Adult Onset Asthma" that is actually undiagnosed COPD, or a combination of the two. Without objective testing, specifically spirometry, clinicians are essentially forced to treat the symptoms and hope for the best.
What this looks like on the ground is a cycle of trial and error. A patient is prescribed an inhaler based on a symptom profile. They return three months later, still breathless. The dose is increased, or a different device is tried. Months, sometimes years, pass before someone asks: "Do we actually have the data to back up this diagnosis?"
By the time that question is asked, the patient may have already suffered irreversible lung damage or spent years on a treatment plan that was never designed for their specific condition.

The "Normalisation" of Breathlessness
One of the most insidious challenges in the current respiratory pathway is the tendency to attribute breathlessness to lifestyle factors or the natural process of aging.
We see this frequently with patients who smoke, those who are living with obesity, or those in their 70s and 80s. There is a systemic bias that suggests if you are 75 and breathless, it’s just "old age." If you smoke and have a cough, it’s just a "smoker’s cough."
This "normalisation" means that patients are entering the system far too late. They aren't being referred for testing until their breathlessness is so profound that it limits their basic activities of daily living. At this stage, the opportunity for early intervention, which is the cornerstone of the NHS Long Term Plan, has already been missed.
We need to move toward a culture where breathlessness is treated as a clinical "red flag" that demands objective investigation, regardless of the patient's age or BMI.
The Spirometry Bottleneck
If the solution is objective testing, why isn't it happening? The reality is that spirometry access in primary care is currently one of the biggest "potholes" in the respiratory pathway.
Since the pandemic, the delivery of spirometry has struggled to return to pre-2020 levels in many regions. Issues with infection control, staff training, and the sheer volume of the backlog have created a "diagnostic desert" in some parts of the UK. When a GP has to wait six months to get a patient in for a spirometry test, the temptation to "treat and see" becomes almost irresistible.
However, treating based on symptoms alone is a false economy. The cost of an incorrect diagnosis, both in terms of medication waste and emergency admissions, far outweighs the cost of providing robust, accessible diagnostic hubs.
Integrated Care Systems (ICSs) are now looking at how to bridge this gap. We are seeing a shift toward "diagnostic hubs" where spirometry, FeNO testing, and other assessments can be centralised. This not only improves accuracy but also relieves the pressure on individual GP practices.

Overlapping Pathogens: Why Symptoms Aren't Enough
Recent surveillance data from the UK Health Security Agency (March 2026) highlights another reason why we can't rely on symptoms alone. We are seeing multiple respiratory pathogens, rhinovirus, hMPV, seasonal coronaviruses, and SARS-CoV-2, all circulating at the same time with significantly overlapping symptoms.
When a patient presents with an acute respiratory episode, it is becoming increasingly difficult to distinguish between a viral flare-up of an existing condition and a new, underlying chronic issue. Clinical indicators often tell a different story than laboratory data. For instance, a patient might "look" like they are having a standard asthma flare, but laboratory swabbing might show a completely different viral driver that requires a different approach to management.
This complexity reinforces the need for a data-driven approach. We need to stop viewing respiratory symptoms in isolation and start looking at them as part of a wider, more complex physiological picture.
Moving Toward Objective Pathways
So, what does pathway transformation actually look like? It starts with moving away from "symptom-based assumptions" and toward "objective-first" protocols.
- Mandatory Diagnostics: No new diagnosis of Asthma or COPD should be confirmed without objective evidence (Spirometry and/or FeNO).
- The "One Airway" View: Recognizing that allergies and rhinitis often drive respiratory symptoms, and testing for these triggers early in the pathway.
- Community Access: Bringing diagnostics closer to the patient to ensure that "lack of access" is no longer an excuse for a "guess."
- Workforce Support: Ensuring that our respiratory nurses and physiotherapists have the time and tools to perform and interpret these tests accurately.
At The Respiratory Network, we believe that collaboration between Life Sciences, the NHS, and patient advocates is the only way to fix these broken links. By sharing data and best practices, we can ensure that the "postcode lottery" of diagnostics becomes a thing of the past.
A Note on Clinical Safety
While we advocate for better pathways and more robust testing, it is vital to remember that every patient is an individual.
The Respiratory Network is not about medical advice. The content here is for informational and networking purposes. If you are concerned about your own health or are experiencing worsening respiratory symptoms, please consult a qualified healthcare professional or your GP.
Join the Conversation
The gap between policy (which calls for early diagnosis) and practice (which often relies on assumptions) is where we lose patients. We want to hear from you: how is your region tackling the diagnostic backlog? Are you seeing the benefits of community diagnostic hubs, or is spirometry still a distant dream for your patients?
We invite you to join the discussion on our Public Forum or connect with other professionals in our Members area.
If you are passionate about shaping the future of NHS respiratory services, consider joining us at our upcoming Round Table event. You can find all the details and secure your place here: The Respiratory Network Round Table 2026.
Let's stop guessing and start testing. The future of the UK respiratory pathway depends on it.
Categories: Pathway Excellence; NHS Strategy & Leadership; Data & Insights
Tags: Respiratory Pathway; NHS Respiratory Services; Spirometry; Diagnostics; COPD; Asthma; ICS; Healthcare Networking UK; NHS Strategy



Responses