

The Breathlessness Syndrome: Why Siloed Care is Failing the Respiratory Pathway

Let’s talk about a scenario that happens every single day in GP surgeries and respiratory clinics across the country. A patient walks in. They’re struggling to catch their breath. They’ve stopped walking to the shops, they can’t play with their grandkids, and they’re scared.
On paper, the system should work. They get a spirometry test. Maybe an inhaler is trialled. But what happens when the spirometry comes back "within normal limits"? Or what happens when the inhaler doesn't quite do the trick? Frequently, this is where the respiratory pathway begins to stutter. The patient is sent back to the GP, perhaps referred to cardiology, or told it might just be "age" or "fitness."
In reality, chronic breathlessness is rarely a single-organ issue. By treating it as a symptom to be filed under a specific department, we are failing to address the complex, multi-faceted reality of respiratory health UK. It’s time we started looking at chronic breathlessness not just as a symptom, but as a clinical syndrome in its own right.
The Diagnostic Merry-Go-Round
The traditional approach to breathlessness is built on silos. If you have a cough and wheeze, you see a respiratory specialist. If you have chest tightness, you see a cardiologist. But the human body doesn’t respect these administrative boundaries.
We know that a significant portion of patients living with chronic breathlessness have "overlap" conditions. You might have mild COPD, but you also have early-stage heart failure. Toss in a bit of anxiety: because, let’s face it, not being able to breathe is terrifying: and suddenly the "standard" pathway feels completely inadequate.
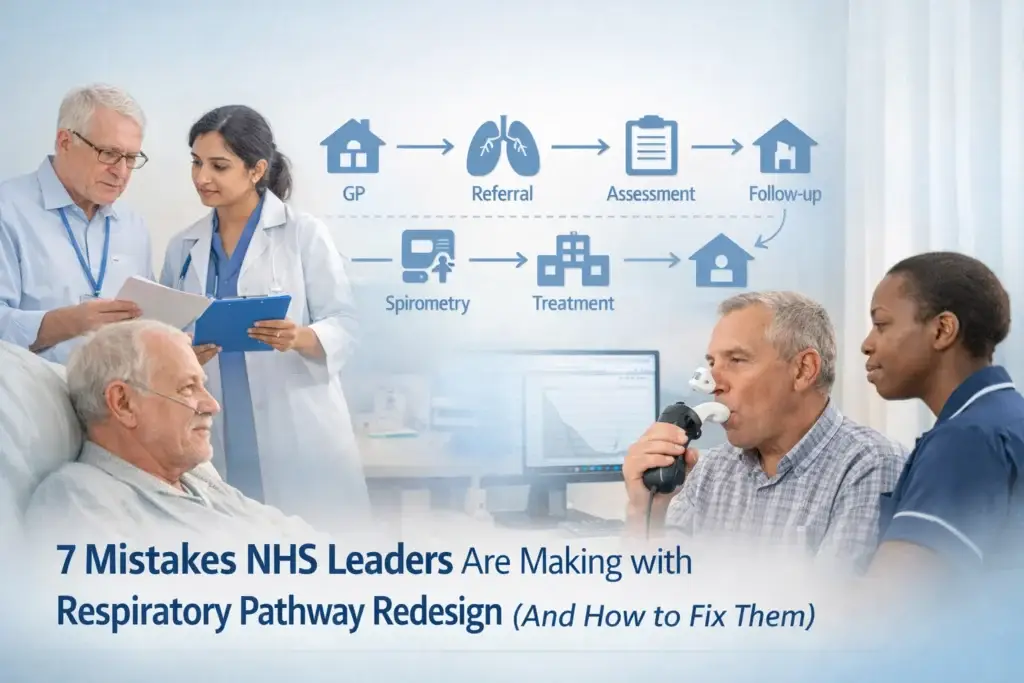
When care is siloed, the patient becomes the project manager of their own illness. They bounce between appointments, repeating their story, while clinicians in different buildings look at different parts of the same puzzle. This "diagnostic merry-go-round" doesn't just waste NHS resources; it delays treatment and allows the disease to progress.
Why "The Breathlessness Syndrome" Matters
If we shifted our perspective and began categorising chronic breathlessness as a clinical syndrome, the entire respiratory pathway would look different. Instead of asking, "Is this a lung problem?" we would start by asking, "Why is this person breathless, and what combination of factors is driving it?"
Treating breathlessness as a syndrome acknowledges three key truths:
- It is multi-factorial: It involves the lungs, the heart, the musculoskeletal system, and the mind.
- It is debilitating: Regardless of the underlying cause, the lived experience of breathlessness is the same. It limits life, reduces physical activity (leading to further deconditioning), and impacts mental wellbeing.
- It requires an integrated response: You cannot "fix" a breathless patient by only looking at one organ through a straw.
In practice, this means moving away from symptom-based assumptions and moving towards objective, holistic testing. What if a patient could attend a single "Breathlessness Hub" where they could access basic diagnostics for both heart and lung health in one go? This isn't just a "nice to have": it’s a necessity for a sustainable NHS.
The "Invisible" Drivers: Anxiety and Deconditioning
One of the biggest gaps in our current respiratory health UK landscape is how we handle the psychological impact of breathlessness. When someone feels they can’t breathe, their sympathetic nervous system goes into overdrive. This creates a vicious cycle: breathlessness leads to anxiety, which causes faster, shallower breathing, which leads to more breathlessness.
In a siloed system, the respiratory nurse might check inhaler technique, but they might not have the time or the specific training to address the panic disorder that has developed alongside the physical condition. Similarly, deconditioning is a massive factor. If it hurts to move, patients stop moving. Their muscles weaken, making even basic tasks more oxygen-demanding.
By treating breathlessness as a syndrome, we can integrate pulmonary rehabilitation and mental health support directly into the primary pathway, rather than as an afterthought or a secondary referral.
What Integrated Care Actually Looks Like
The rise of Integrated Care Systems (ICS) gives us a unique opportunity to redesign these pathways. But "integration" shouldn't just be a buzzword on a PowerPoint slide. What this looks like on the ground is a shift in how we fund and staff our services.
We need to empower our multidisciplinary teams (MDTs). This means bringing together respiratory specialists, cardiologists, physiotherapists, and mental health practitioners to review complex cases collectively. It’s about creating a system where the data flows as easily as the patient should be breathing.

For the Life Sciences sector, this shift presents a call to action. We don't just need better medications; we need better diagnostic tools and digital solutions that help clinicians monitor these "overlap" patients in real-time. Smart monitoring that tracks both heart rate and respiratory rate can provide a much clearer picture of what is happening during an exacerbation than a snapshot taken in a clinic every six months.
The Economic Argument
Some might argue that creating integrated breathlessness clinics is too expensive. However, the cost of not doing it is much higher.
Think about the number of A&E admissions caused by "unspecified breathlessness." Think about the repeated GP appointments, the duplicate tests, and the long-term cost of patients who become housebound and require social care because their condition wasn't managed holistically five years ago.
By intervening early with a "Breathlessness Syndrome" mindset, we can keep patients active, reduce the burden on emergency services, and improve the overall quality of life for millions.
Moving the Needle
We know the workforce is stretched. We know that respiratory nurses are doing the work of three people. That’s why pathway redesign isn't about asking staff to do more; it’s about asking the system to work smarter.
If we can streamline the diagnostic process and stop patients from falling through the gaps between specialties, we actually free up capacity. We move from a reactive system that puts out fires to a proactive one that manages health.

A Final Note on Medical Advice
Important Note: The content provided in this blog is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions you may have regarding a medical condition. We do not recommend specific medications or drug treatments; management should always be tailored to the individual by a clinical professional.
Join the Conversation
The "Mind the Gap" theme is something we live and breathe at The Respiratory Network. We believe that the only way to truly transform respiratory health UK is to get the right people in the room: clinicians, patients, and industry leaders: and have the difficult conversations about why the current respiratory pathway is failing some of our most vulnerable patients.
Are you seeing the impact of siloed care in your neck of the woods? We want to hear from you.
- Become a Member: Join our growing community of professionals and advocates working to change the face of respiratory care. Register here.
- Join the Discussion: Head over to our public forums to share your thoughts on the "Breathlessness Syndrome" concept.
- Attend Our Round Table: We are hosting a deep dive into pathway innovation at The King's Fund on the 29th of April. This is where the real work happens. Find out more and book your spot.
Let's stop treating the lungs in isolation and start treating the person who is fighting for their next breath. It's time to bridge the gap.



Responses