

The Blue Inhaler Trap: Why "Just a Quick Puff" Can Hide Poor Asthma Control

Medical Disclaimer: This article provides general information about asthma management and is not a substitute for professional medical advice. If you are experiencing severe breathlessness, chest tightness, or symptoms that are not relieved by your usual treatment, seek urgent medical attention. For questions about your asthma treatment or inhaler use, please contact your GP, asthma nurse, or healthcare provider.
In GP surgeries, community pharmacies and respiratory clinics across the UK, the blue reliever inhaler remains one of the most recognised symbols of asthma care. For many people, it represents quick relief when breathing becomes difficult. But increasingly, that familiar blue device is also becoming a warning sign of something more concerning: poorly controlled asthma that's being masked rather than managed.
The pattern is well established in clinical practice. A patient requests another blue inhaler prescription. Then another. Perhaps they mention needing it "just to get through the day" or using it before exercise, before bed, when the weather changes. What looks like responsible symptom management is often the opposite. Frequent use of a blue reliever without appropriate anti-inflammatory treatment is now recognised as one of the clearest indicators that asthma control has deteriorated.
This matters because the relief these inhalers provide is temporary. They open airways quickly, but they do nothing to address the underlying inflammation that causes asthma symptoms in the first place. And while the patient feels better in the short term, the condition itself continues to worsen beneath the surface.
What the Blue Inhaler Actually Does
Blue reliever inhalers contain short-acting bronchodilators, typically salbutamol or terbutaline. These medications work by relaxing the muscles around the airways, allowing them to open and making it easier to breathe. The effect is fast, usually within five to ten minutes, and for someone experiencing tightness or wheeze, that relief is significant.

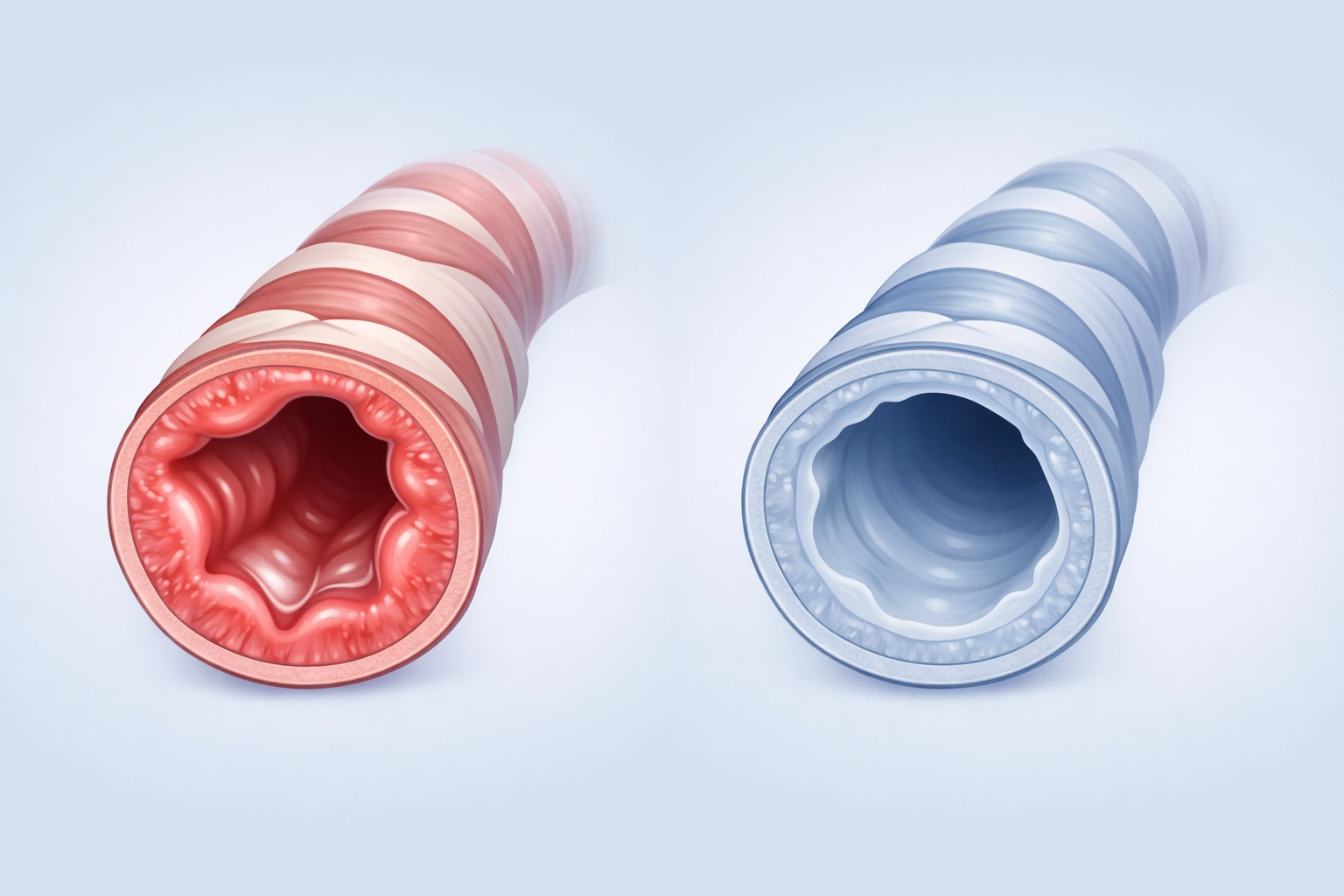
But relief is not the same as control. Asthma is driven by chronic inflammation in the airways. That inflammation makes the airways more sensitive, more likely to narrow in response to triggers, and more prone to producing excess mucus. A blue inhaler does not reduce inflammation. It simply counteracts the tightening of the airways caused by it.
In practice, this means that someone relying heavily on their blue inhaler is treating the symptom but not the disease. The inflammation remains. The risk of a serious asthma attack remains. And over time, the frequency of symptoms often increases because the underlying problem is never addressed.
When Relief Becomes a Red Flag
Current clinical guidance is clear: using a blue reliever inhaler more than two to three times per week suggests that asthma is not well controlled. Purchasing three or more blue inhalers in a year is considered overuse. Yet this pattern is common, and not always recognised as a concern by the person living with it.
What patients and clinicians often describe is a gradual normalisation of symptoms. The blue inhaler becomes part of the routine. It's used before leaving the house, before going to sleep, during conversations, after climbing stairs. The person adapts to needing it, rather than questioning why they need it so often.
From a clinical perspective, this frequent use without adequate anti-inflammatory treatment is not just ineffective. It is actively associated with worse outcomes. Research has consistently shown that reliance on short-acting bronchodilators alone increases the risk of asthma attacks, emergency hospital admissions, and in the most serious cases, asthma-related deaths.
The trap is in the relief itself. Because the inhaler works quickly, it creates the impression that the asthma is being managed. Symptoms are dealt with as they arise. But asthma care is not meant to be reactive in this way. The goal is prevention, not repeated rescue.
The Role of Preventer Treatment
The evidence base for inhaled corticosteroids in asthma management is long established. These preventer inhalers, often brown or orange, work by reducing inflammation in the airways over time. They do not provide immediate relief, which is why adherence can be inconsistent. But when used regularly, they significantly reduce the frequency and severity of symptoms, lower the risk of asthma attacks, and reduce the need for reliever medication.

For many people with asthma, the recommended approach is daily use of a preventer inhaler, alongside a blue reliever kept for occasional use when symptoms break through. In recent years, guidance has shifted further towards combination inhalers that contain both an anti-inflammatory steroid and a bronchodilator in a single device. These are used both as a preventer and as a reliever, and have been shown to reduce the risk of severe asthma attacks compared to blue inhalers used alone.
Yet adherence to preventer therapy remains a widespread challenge. People stop using inhalers when they feel well. They forget doses. They dislike the idea of taking medication every day for a condition that feels intermittent. And when symptoms return, they reach for the blue inhaler because it works immediately.
This is where system design matters. If a patient only ever receives a blue inhaler without structured review, without education about inflammation, without a written asthma action plan, then the default becomes reactive management. The blue inhaler becomes the treatment, rather than a safety net.
A System-Wide Pattern
From the perspective of NHS respiratory leads and commissioners, the overuse of short-acting bronchodilators is not just a clinical issue. It is a service design issue. High rates of blue inhaler prescribing without corresponding preventer use suggest gaps in structured asthma care. They indicate missed opportunities for review, education and optimisation of treatment.
For Life Sciences partners working in respiratory care, this pattern also represents a disconnect between available evidence and real-world practice. Effective treatments exist. Guidelines are clear. Yet implementation across primary care, community pharmacy and secondary care remains inconsistent. Supporting pathway change requires understanding not just the clinical evidence, but the practical barriers to delivering it at scale.
What this looks like on the ground is variation. Some practices conduct regular asthma reviews with dedicated nursing time. Others rely on opportunistic consultations during acute presentations. Some areas have integrated respiratory hubs with access to spirometry and specialist advice. Others do not. And in that variation, patients experience very different standards of care.
The blue inhaler becomes a symbol of that inconsistency. It is universally available, easy to prescribe, and meets an immediate need. But without the surrounding infrastructure of review, education and access to preventers, it also perpetuates a cycle of poor control.
What Needs to Change
Addressing the blue inhaler trap requires action at multiple levels. At the individual level, it means ensuring that everyone with asthma has access to a structured review at least annually, with an up-to-date written asthma action plan that explains when to step up treatment and when to seek urgent care.
At the practice level, it means using prescribing data to identify patients who may be overusing reliever inhalers and proactively inviting them for review. It means embedding preventer use as the foundation of asthma care, and ensuring that patients understand why daily treatment matters even when they feel well.
At the system level, it means commissioning pathways that support good asthma care, with accessible diagnostics, clear referral routes, and time protected for respiratory nurses to deliver structured reviews. And it means ensuring that community pharmacies, which are often the first point of contact when someone requests another blue inhaler, are supported to ask the right questions and signpost to appropriate care.
For industry, it means moving beyond simply supplying inhalers and towards supporting system change. That includes educational initiatives for clinicians, patient-facing resources that explain the difference between relievers and preventers, and collaboration with NHS partners to redesign pathways that make good care the default.
Why This Matters to The Respiratory Network
At The Respiratory Network, we bring together NHS leaders, clinicians, Life Sciences partners and patient advocates precisely because challenges like the blue inhaler trap cannot be solved in isolation. They require shared understanding of the clinical evidence, the practical constraints within the NHS, the lived experience of people managing asthma, and the role that industry can play in supporting change.
Our roundtable discussions and community forums create space for those conversations. We hear from respiratory leads managing stretched budgets and workforce pressures. We hear from patients navigating inconsistent access to specialist care. We hear from Life Sciences teams working to align innovation with real-world implementation challenges.

The blue inhaler trap is not a failure of individual patients or individual clinicians. It is a system-level issue that reflects the way asthma care has been structured, resourced and delivered. Changing that requires collaboration, and it requires the kind of practical, grounded conversations that move beyond guidelines and towards implementation.
If you are working in respiratory care, whether as a clinician, commissioner, industry partner or patient advocate, we would welcome your involvement. Our upcoming roundtable events focus specifically on translating evidence into practice, and our community forums provide ongoing space for shared learning.
You can register here to join the network, or visit our news section to stay informed about developments in respiratory care across the UK.
The Path Forward
The blue inhaler is not the problem. The problem is a system that allows it to be used as a substitute for proper asthma control rather than as part of a structured treatment plan. Changing that requires better data, better pathways, better education and better collaboration across the respiratory ecosystem.
For every patient reaching for their blue inhaler multiple times a day, there is an opportunity. An opportunity to ask better questions. An opportunity to offer better treatment. An opportunity to prevent the next asthma attack before it happens.
That is the work ahead. And it is work that requires all of us.
Full Medical Disclaimer:
This article is intended for general informational and educational purposes only and does not constitute medical advice, diagnosis, or treatment. The content provided is based on current clinical guidelines and evidence available at the time of writing, but individual circumstances vary significantly.
Do not use this article to self-diagnose or change your asthma treatment without consulting a qualified healthcare professional. Asthma is a serious condition that requires personalised medical assessment and ongoing monitoring by a GP, asthma nurse, respiratory specialist, or other qualified healthcare provider.
If you are experiencing any of the following, seek urgent medical attention immediately:
- Severe breathlessness or difficulty speaking in full sentences
- Blue lips or fingernails
- Feeling exhausted or unable to manage symptoms
- No improvement after using your reliever inhaler
- Symptoms rapidly worsening
For non-urgent concerns about your asthma treatment, inhaler technique, or medication use, please contact your GP surgery, asthma nurse, or NHS 111 for advice.
The Respiratory Network does not provide clinical services or individual medical advice. We are a professional networking and engagement organisation connecting NHS professionals, Life Sciences partners, and patient advocates across the UK respiratory community.
Always follow the specific treatment plan provided by your healthcare team, and attend regular asthma reviews as recommended. For more information about asthma management, visit www.asthma.org.uk or speak to your healthcare provider.




Responses