

The Spirometry Bottleneck: Why Quality-Assured Testing Is the Unsung Hero of Respiratory Care in 2026

If you've spent any time working in respiratory care over the past two years, you've probably heard spirometry described as both "essential" and "underutilised" in the same breath. It's the diagnostic cornerstone for COPD and asthma, yet access remains patchy, quality varies wildly, and the pathway between test and treatment still feels frustratingly slow.
By 2026, we're at an inflection point. Quality-assured spirometry isn't just nice to have anymore. It's the difference between catching disease early and watching patients deteriorate. Between confident diagnosis and best-guess treatment. Between data that drives decisions and numbers that don't mean much at all.
So why does it still feel like we're waiting for something to shift?
What's Actually Happening on the Ground
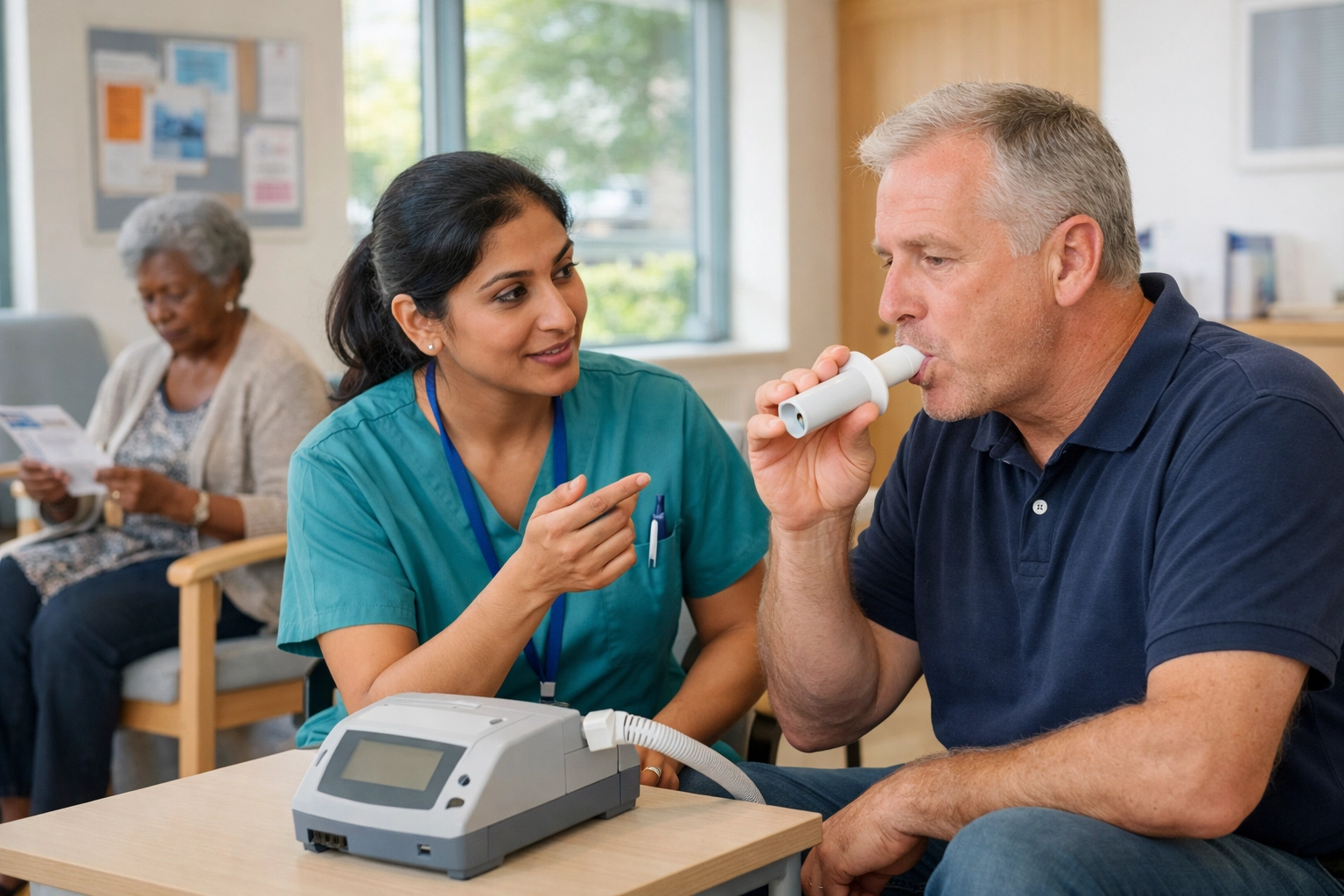
In practice, spirometry should be straightforward. A patient blows into a device. Lung function gets measured. Clinicians use those numbers to diagnose, monitor, or adjust treatment. Simple.
Except it's not.
The testing environment matters. The technician's training matters. Calibration matters. Whether the patient understands what they're doing, and whether they can do it properly, matters enormously. A poorly conducted spirometry test isn't just unhelpful. It's actively misleading.

What patients and clinicians often describe is a system where spirometry availability depends heavily on geography and capacity. Some GP surgeries have well-maintained equipment and trained staff. Others refer out to community clinics or hospitals, adding weeks to the pathway. In some areas, patients wait months for a test that takes ten minutes to perform.
Quality assurance doesn't fix capacity. But it does ensure that when a test happens, it's worth doing.
The Regulatory Reality
Here's where it gets complicated, and expensive.
Spirometry devices need regulatory approval to be used in clinical settings. In the UK and Europe, that means meeting CE MDR standards. In the US, it's FDA 510(k). In other markets, different bodies with different requirements. For manufacturers, particularly smaller innovators, meeting these standards is resource-intensive. It's why incumbents dominate, and why genuinely new approaches to outpatient diagnostics struggle to reach the market.
In 2025, the FDA cleared 14 AI-enabled spirometry platforms. Early detection sensitivity for COPD sat at 91%. That's promising. But regulatory approval is only the start. Getting those devices into NHS pathways, ensuring they're reimbursed, training staff to use them, and proving their value in real-world settings, that's the longer game.
What this looks like on the ground is a gap between what's technically possible and what's practically available. Clinicians know better tools exist. Patients hear about innovation. But the procurement cycle, budget constraints, and existing contracts mean adoption lags behind capability.
The Shift to Distributed Testing
Spirometry used to live in hospital respiratory labs and specialist clinics. Controlled environments. Trained technicians. Regular calibration. Quality baked in.
Now, spirometry is moving outward, into GP surgeries, community hubs, pharmacies, and eventually homes. That shift is necessary. It improves access, reduces waiting times, and meets patients where they are. But it also introduces risk.
When spirometry moves to distributed settings, quality control becomes harder to maintain. Who calibrates the device? How often? Who ensures the person conducting the test follows the right protocol? What happens when a reading looks wrong, does anyone notice?
In pediatric asthma studies, home-based monitoring showed compliance dropping from 80% to around 50% after twelve weeks. Patients stop engaging. Devices sit unused. Data gaps appear. The promise of continuous monitoring hits the reality of daily life.
This isn't a technology problem. It's a human one. Quality-assured spirometry in distributed settings requires more than good devices. It requires training, support, follow-up, and systems that catch errors before they matter.
What Quality Assurance Actually Means
Quality assurance in spirometry isn't bureaucratic box-ticking. It's the stuff that makes a test reliable.
It means:
- Devices are calibrated regularly, not "when we remember"
- Technicians follow standardised protocols, not their own interpretation
- Results are reviewed by someone who knows what they're looking at
- Poor-quality tests are flagged and repeated, not accepted and filed
In a hospital lab, this infrastructure exists. In a busy GP surgery or a patient's living room, it's much harder to sustain.
The 2027 expectation, shared by healthcare systems and device manufacturers, is that AI-driven spirometry and remote monitoring will transition from pilot programmes to standard care pathways. That's not far off. But the gap between "technically ready" and "systematically embedded" is significant.
What patients and clinicians need is clarity. Who owns quality when testing happens outside traditional settings? How do we prove a home spirometry reading is as reliable as one done in clinic? And when something goes wrong, who's accountable?
The NHS Context
Let's be honest about where NHS respiratory services are right now. Capacity is tight. Budgets are tighter. Staff are managing impossibly high caseloads. Adding "ensure spirometry quality assurance" to an already overloaded to-do list feels unrealistic.
But here's the thing: poor-quality spirometry creates more work, not less. Incorrect diagnoses lead to inappropriate treatment. Missed early disease means more acute admissions later. Inconsistent monitoring means reactive rather than proactive care.
Quality-assured spirometry isn't an add-on. It's a foundation. Without it, everything built on top, treatment pathways, remote monitoring, early intervention strategies, sits on shaky ground.

Integrated Care Systems are starting to recognise this. Some are investing in standardised training. Others are piloting digital spirometry with built-in quality checks. A few are exploring shared services, where spirometry expertise is pooled across primary and secondary care.
None of this happens quickly. But the direction is clear.
The Life Sciences Piece
For Life Sciences, quality-assured spirometry presents both opportunity and responsibility.
The opportunity is obvious. Better diagnostics mean better patient identification. Better monitoring means better evidence for therapies. Devices that integrate seamlessly into care pathways make everyone's life easier.
The responsibility is less often discussed. If manufacturers want their spirometry devices adopted across the NHS, they need to think beyond the sale. What training do they provide? What quality assurance processes are built into the device itself? How easy is it for a non-specialist to use correctly?
In practice, the best partnerships happen when Life Sciences sits alongside NHS teams and asks, "What would make this actually work for you?" Not, "Here's our solution: make it fit."
What Happens Next
By the end of 2027, quality-assured spirometry will either be standard practice or still stuck in the "should happen" category. The difference will come down to decisions made now.
That means procurement teams prioritising quality alongside cost. It means commissioners building spirometry standards into pathway redesign. It means clinicians being supported: not just expected: to deliver high-quality testing. And it means patients understanding why a repeat test, or a different testing environment, isn't an inconvenience: it's good medicine.
None of this is glamorous. But it matters.
Join the Conversation
If you're working on diagnostics, respiratory pathways, or trying to make spirometry work better in your system, you're not alone. The Respiratory Network brings together NHS professionals, Life Sciences partners, and patient advocates who understand that better care starts with better foundations.
Register to join the community, share what's working (and what isn't), and help shape the next generation of respiratory diagnostics. Or join us at our Round Table event to dig into these challenges with people who get it.
Quality-assured spirometry won't fix everything. But it's a start. And in 2026, we need to start somewhere.



Responses