

Is it COPD, Asthma, or CF? Navigating Diagnosis and the NICE Guidelines
In the current UK healthcare landscape, the respiratory pathway is under more pressure than ever. For NHS respiratory leadership, the challenge is not just managing volume, but ensuring diagnostic accuracy in an environment where symptoms often refuse to sit neatly within a single box. Breathlessness, a chronic cough, and frequent exacerbations are the "bread and butter" of respiratory clinics, yet they form a diagnostic Venn diagram where Chronic Obstructive Pulmonary Disease (COPD), Asthma, and Cystic Fibrosis (CF) frequently overlap.
Before we delve into the clinical distinctions and guidelines, please note this blog post is for informational and educational purposes only. It does not constitute medical advice, legal advice, or clinical diagnostic instruction. Always consult with a qualified healthcare professional regarding specific patient cases or personal health concerns.
The Complexity of the Respiratory Pathway
In practice, the journey from a patient’s first primary care appointment to a definitive secondary care diagnosis can be long and winding. What looks like "difficult asthma" may, upon closer inspection, be adult-presentation Cystic Fibrosis. What is recorded as "smoker's cough" or COPD might actually be an underlying fibrotic condition or even bronchiectasis related to CF.
For those involved in life sciences engagement in the UK, understanding these nuances is critical. It is no longer enough to provide a solution for a single disease state; the goal is to support a more integrated, accurate respiratory pathway that identifies the right patient for the right intervention at the earliest possible stage.
Cystic Fibrosis vs. Asthma: The Diagnostic Trap
Asthma is one of the most common respiratory conditions in the UK, but its prevalence can sometimes lead to "diagnostic overshadowing." Because both asthma and CF involve airway inflammation and obstruction, they can appear remarkably similar on a spirometry report.
According to research published in journals such as The Lancet Respiratory Medicine, approximately 37% of patients with Cystic Fibrosis also meet the clinical criteria for asthma. This coexistence makes the differential diagnosis particularly difficult. However, the underlying mechanisms differ significantly. While asthma is often driven by a hypersensitivity to allergens or environmental triggers, the inflammation in CF is frequently linked to a genetic defect in the CFTR protein, leading to thick, dehydrated mucus and a high susceptibility to specific infections, such as mold and fungi.
Key Distinctions:
- The Sweat Test: NICE Guideline [NG78] remains the gold standard for CF diagnosis. A sweat chloride test (values ≥60 mmol/L) is a definitive marker for CF, whereas asthma patients will typically show normal results.
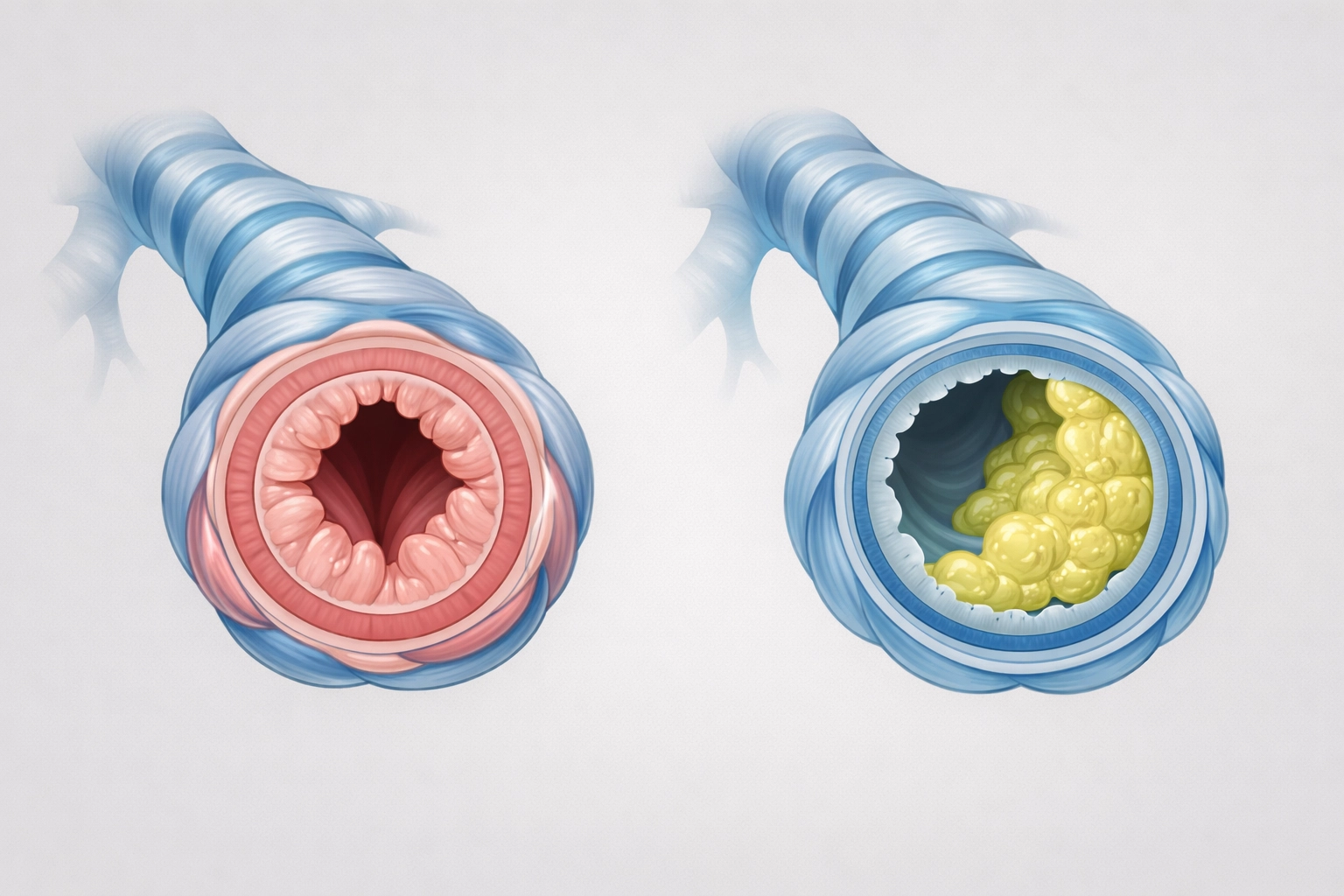
- Mucus Consistency: In practice, CF is characterized by "sticky" mucus that is difficult to clear, leading to permanent structural changes known as bronchiectasis.
- Treatment Response: If a patient with an asthma diagnosis fails to respond to standard maintenance therapy, clinical leads often flag this as a "red light" to investigate for CF or other underlying pathologies.
What is Commonly Mistaken for COPD?
COPD is often the "default" diagnosis for older adults with a history of smoking who present with progressive breathlessness. However, several conditions are commonly mistaken for COPD, leading to delays in appropriate management.
- Bronchiectasis: Often occurring alongside or instead of COPD, this involves permanent enlargement of parts of the airways.
- Cystic Fibrosis (Adult Presentation): While CF is usually diagnosed in childhood through newborn screening, some individuals with "milder" genetic mutations may not show significant symptoms until adulthood, where they are frequently mislabelled as having COPD or chronic bronchitis.
- Heart Failure: The symptomatic overlap between cardiac breathlessness and respiratory breathlessness remains a significant hurdle in the NHS respiratory pathway.
In the context of Cystic Fibrosis and COPD, the distinction usually lies in the multi-system nature of CF. While COPD is primarily a disease of the lungs (though with systemic inflammatory effects), CF affects the pancreas, digestive system, and sweat glands. A patient presenting with respiratory issues alongside digestive complications or unexpected weight loss should be screened for CF, regardless of their age or smoking history.
Cystic Fibrosis vs. Pulmonary Fibrosis
While both contain the word "fibrosis," these two conditions sit at different ends of the respiratory spectrum.
- Cystic Fibrosis is an obstructive disease. The primary issue is the blockage of airways by mucus and subsequent infection. The "fibrosis" in CF refers to the scarring that occurs in the lungs and the pancreas due to chronic inflammation and repeated infections.
- Pulmonary Fibrosis (such as Idiopathic Pulmonary Fibrosis or IPF) is a restrictive disease. The primary issue is the thickening and stiffening of the lung tissue itself, making it difficult for the lungs to expand.
Clinicians often use high-resolution computed tomography (HRCT) to distinguish between the two. In CF, the scans typically show bronchiectasis and mucus plugging. In Pulmonary Fibrosis, the scans show a "honeycombing" pattern of scarred tissue.

Navigating the NICE Guidelines (NG78, NG80, and NG115)
For NHS respiratory leadership, the NICE guidelines provide the framework for reducing diagnostic error.
- NICE [NG115] (COPD): Emphasises the use of post-bronchodilator spirometry to confirm airflow obstruction that is not fully reversible.
- NICE [NG80] (Asthma): Focuses on a combination of clinical history, spirometry, and FeNO (fractional exhaled nitric oxide) testing to identify eosinophilic inflammation.
- NICE [NG78] (Cystic Fibrosis): Outlines the necessity of genetic testing and sweat testing for anyone with symptoms suggestive of CF, including those with persistent chest infections or malabsorption.
The challenge on the ground is that these guidelines are often implemented in silos. A more integrated approach: one that considers the "whole patient": is essential for improving outcomes. This is where life sciences engagement in the UK plays a pivotal role. By supporting the development of better diagnostic tools and more efficient pathways, industry partners can help the NHS move from "managing symptoms" to "managing the specific disease."
What This Looks Like on the Ground
In practice, a well-functioning respiratory pathway relies on the ability of clinicians to step back and question an initial diagnosis when a patient is not progressing as expected. What patients and clinicians often describe is a feeling of being "stuck" in a treatment cycle that isn't working.
For instance, a patient might be prescribed multiple inhalers for what is thought to be COPD. If their lung function continues to decline rapidly and they are producing high volumes of purulent sputum, the pathway should pivot toward investigating CF or bronchiectasis.
From a Life Sciences perspective, this highlights the need for data-driven insights. Understanding the prevalence of misdiagnosis helps in tailoring educational support for HCPs and ensuring that the right therapies: whether they be mucus-clearing agents, specialized antibiotics, or advanced biologics: are reaching the patients who actually need them.

Conclusion: Moving Toward Diagnostic Precision
The overlap between COPD, asthma, and cystic fibrosis is a clinical reality that requires a high index of suspicion and a commitment to the NICE frameworks. For the NHS, the goal is to ensure that no patient is "lost" behind an incorrect label. For Life Sciences, the opportunity lies in supporting this diagnostic journey through better evidence, better engagement, and a deeper understanding of the system's pressures.
Improving the respiratory pathway is not just about new treatments; it is about the clinical leadership required to refine how we identify these diseases in the first place. When we get the diagnosis right, we don't just improve a metric: we fundamentally change the trajectory of a person’s life.
Join the Conversation
Are you a clinical lead, a patient advocate, or a professional in the Life Sciences sector looking to improve respiratory outcomes in the UK? We invite you to be part of the solution.
- Become a Member: Connect with a network of experts dedicated to respiratory excellence. Join us here.
- Follow Our Insights: Stay updated on the latest shifts in the NHS respiratory landscape via our news feed.
- Attend Our Events: Participate in high-level discussions that bridge the gap between policy and practice. View our upcoming topics.
Together, we can build a respiratory pathway that is as precise as it is compassionate.



Responses