

The Invisible COPD Struggle: What Life is Really Like Beyond the Breathlessness
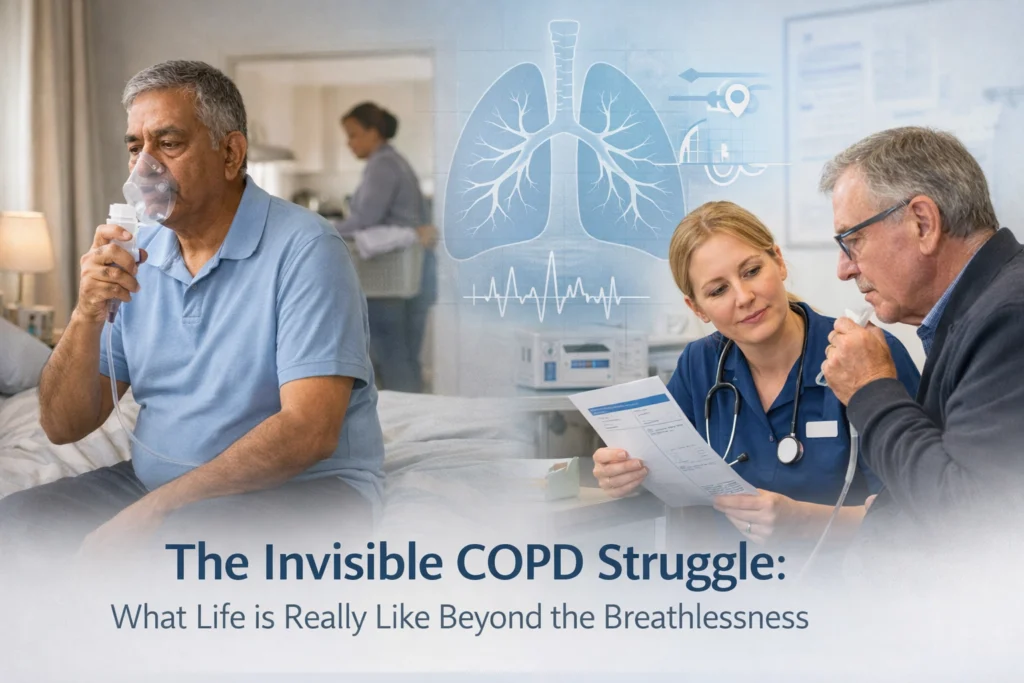
When most people think about COPD, they picture someone gasping for breath or reliant on oxygen. What they don't see is the person rationing energy to wash their hair. The one who cancels plans not because they're breathless, but because the anxiety of potentially becoming breathless is paralysing. Or the patient who looks perfectly well in the GP surgery but hasn't left their house unaccompanied in six months.
COPD is often described as an invisible illness, not because the disease itself is hidden, but because so many of its impacts don't show up on a spirometry reading or in a hospital corridor. And that invisibility creates a gap between what patients experience and what those around them understand.
The Paradox of Looking Fine
One of the most isolating aspects of living with COPD is how often you don't look unwell. Patients describe this repeatedly: they might be managing day-to-day with careful planning, pacing and medication adherence, but to an outsider, they appear healthy. Even in moderate to severe COPD, breathlessness itself can be invisible, until it suddenly isn't.
In practice, this creates a disconnect. Family members, colleagues, even some clinicians may struggle to grasp why someone who "seems fine" can't manage a flight of stairs, attend a social event or hold down full-time work. Patients report feeling doubted, dismissed or misunderstood, not maliciously, but because their external appearance doesn't match their internal reality.
This is compounded by the unpredictable nature of exacerbations. Someone can be stable one week and in crisis the next. The lack of visible warning signs makes it hard for others to anticipate or respond appropriately, leaving patients feeling unsupported when they need it most.

The Mental Health Toll No One Talks About
What often goes unspoken in respiratory clinics is the psychological weight of living with progressive breathlessness. Patients describe a constant, low-level fear, not just of the next exacerbation, but of suffocation itself. Many report intrusive thoughts about dying, particularly at night when lying flat worsens dyspnoea.
This isn't anxiety in the traditional sense. It's a rational response to a frightening symptom that, by its nature, feels life-threatening. But because breathlessness is so poorly understood by those who haven't experienced it, patients often feel their distress is minimised or pathologised rather than acknowledged as a legitimate part of their condition.
Depression and COPD are closely linked, and not just because of the physiological overlap. The loss of function, being unable to work, socialise or care for grandchildren, erodes a person's sense of purpose and identity. Patients describe feeling like a burden, particularly when they need help with tasks they used to manage independently.
What clinicians and loved ones often miss is that this psychological suffering is not secondary to COPD, it's part of the disease experience. And it compounds physical symptoms. Anxiety worsens breathlessness. Isolation worsens mood. Fatigue worsens both. It's a cycle that's hard to break without addressing the emotional landscape alongside the clinical one.
The Exhaustion That Doesn't Show
Fatigue is one of the most common yet least recognised symptoms of COPD. It's not the kind of tiredness that improves with a good night's sleep. It's bone-deep, relentless and disproportionate to physical exertion.
Patients describe having to ration energy in ways that are invisible to others. Choosing between a shower or cooking dinner. Needing a full day to recover from a routine GP appointment. Planning every outing around where they can sit down, how far they'll need to walk and whether there will be stairs.
This energy rationing becomes a form of grief. People mourn the spontaneity they've lost, the ability to say yes without mentally calculating oxygen reserves. And because they've learned to manage within their limits, others assume they're coping well. In reality, they're just very good at hiding how much effort it takes to appear functional.
The invisibility of this exhaustion also makes it difficult to access support. Disability assessments and benefits systems often focus on what someone can't do at all, rather than what they can only do at significant physical and emotional cost. Many patients with COPD fall into a gap, too unwell to work, but not obviously disabled enough to qualify for financial or practical help.

Social Isolation and the Shrinking World
As COPD progresses, many patients describe their world becoming smaller. Not all at once, but incrementally. First, they stop going upstairs unnecessarily. Then they avoid crowded places where people might smoke or wear strong perfume. Eventually, some find it easier not to leave the house at all.
This isolation is rarely a choice. It's driven by a combination of physical limitation, fear of exacerbation and the emotional toll of repeatedly explaining why they can't do things that look easy. Patients report feeling left out of family events, friendships fading and a growing sense of being forgotten.
What loved ones and clinicians sometimes miss is that isolation isn't just about mobility. It's about the unshareability of breathlessness, the impossibility of conveying what it feels like to someone who's never experienced it. Patients describe a profound loneliness that comes from living with something others can't see or fully understand.
In practice, this means that asking "How are you managing?" in a ten-minute consultation rarely surfaces the extent of someone's isolation. Patients have learned that people don't really want the full answer. So they say they're fine, and the opportunity to intervene is missed.
The Early-Stage Invisibility
Mild COPD is particularly poorly understood. Patients in the early stages often don't look unwell at all, yet they're already making significant lifestyle adjustments, avoiding triggers, managing anxiety about progression, navigating the emotional impact of a chronic diagnosis.
These patients describe feeling dismissed or told they're worrying unnecessarily. But in reality, they're at a critical juncture. Early intervention, smoking cessation, pulmonary rehab, self-management education, can make a real difference to long-term outcomes. But if the invisibility of their symptoms leads to their concerns being minimised, those opportunities are lost.
What patients and clinicians often describe is a mismatch between symptom severity and life impact. Someone with mild airflow limitation might still be profoundly affected by breathlessness, fatigue or fear. Spirometry results don't capture that.

What This Means for Care
If we accept that COPD's most debilitating impacts are often invisible, then we have to rethink how we assess, support and communicate with patients.
In practice, that means:
- Asking not just about breathlessness, but about how someone's day-to-day life has changed
- Recognising that mental health support isn't a nice-to-have, it's core to respiratory care
- Understanding that someone who looks well may still be struggling significantly
- Creating space in consultations for patients to describe the things they're not asked about directly
It also means better education for families, carers and employers. The more people understand what living with COPD actually looks like, the less isolated patients will feel.
A Note on Medical Advice
This article reflects commonly described experiences of living with COPD, but it is not medical advice. If you're experiencing worsening breathlessness, new or persistent symptoms, or significant changes to your mental health, please speak to your GP or respiratory team. Everyone's experience of COPD is different, and management should always be tailored to your individual circumstances by a qualified healthcare professional.
The Conversations We Need to Have
The invisibility of COPD isn't something we can fix with better diagnostics or more funding alone. It requires a cultural shift: one where we acknowledge that serious illness doesn't always look serious, and that struggling doesn't always look dramatic.
Patients, clinicians and Life Sciences all have a role to play in closing the gap between what COPD looks like and what it feels like. That starts with listening, believing and recognising that the most significant impacts of this disease are often the ones no one sees.
If you're working to improve respiratory care pathways or want to be part of conversations that centre lived experience alongside clinical and strategic insight, join The Respiratory Network. We're bringing together patients, clinicians and industry to rethink what good respiratory care looks like: starting with the realities that too often go unseen.
Follow us on social media for more insight, or explore our upcoming Round Table events where these conversations happen in practice.




Responses