

Sleep, Lungs, and Everything in Between: Why a Good Night’s Rest is a Team Effort
Disclaimer: The Respiratory Network provides information and insight for educational purposes only. This content does not constitute medical advice, diagnosis, or treatment. If you have questions about your health or symptoms, please speak to a qualified healthcare professional.
As we look ahead to the 24th of June for The Respiratory Network’s Round Table event, there is a specific topic that often hums in the background of our clinical and personal conversations: sleep. It is the quiet foundation of respiratory health, yet it is frequently one of the most complex puzzles to solve for patients and clinicians alike.
When we talk about lung health, we often focus on the waking hours, the breathlessness during a walk to the shops, the cough that interrupts a meeting, or the struggle to climb a flight of stairs. But what happens when the sun goes down is just as critical. Sleep isn’t just a period of inactivity; for the respiratory system, it’s a shift change where the body’s mechanics alter, and the environment around us begins to play a much larger role.
Before we dive into the nuances of rest, it’s important to share a note from our colleague, Linda. As she often reminds us, the information shared here is for insight and discussion purposes within our network; it isn’t medical advice. If you’re struggling with your health or sleep quality, please do reach out to your clinical team. Additionally, you’ll notice we won’t be mentioning any specific medications or drug names here: our focus is on the pathway, the environment, and the collaborative effort of care.
The Night Shift: What Happens to Our Lungs?
In practice, the way we breathe changes the moment we drift off. Our breathing rate slows, our muscles relax, and for those living with chronic respiratory conditions, these natural shifts can sometimes create a perfect storm. What might be a minor irritation during the day can become a significant barrier to restorative rest at night.
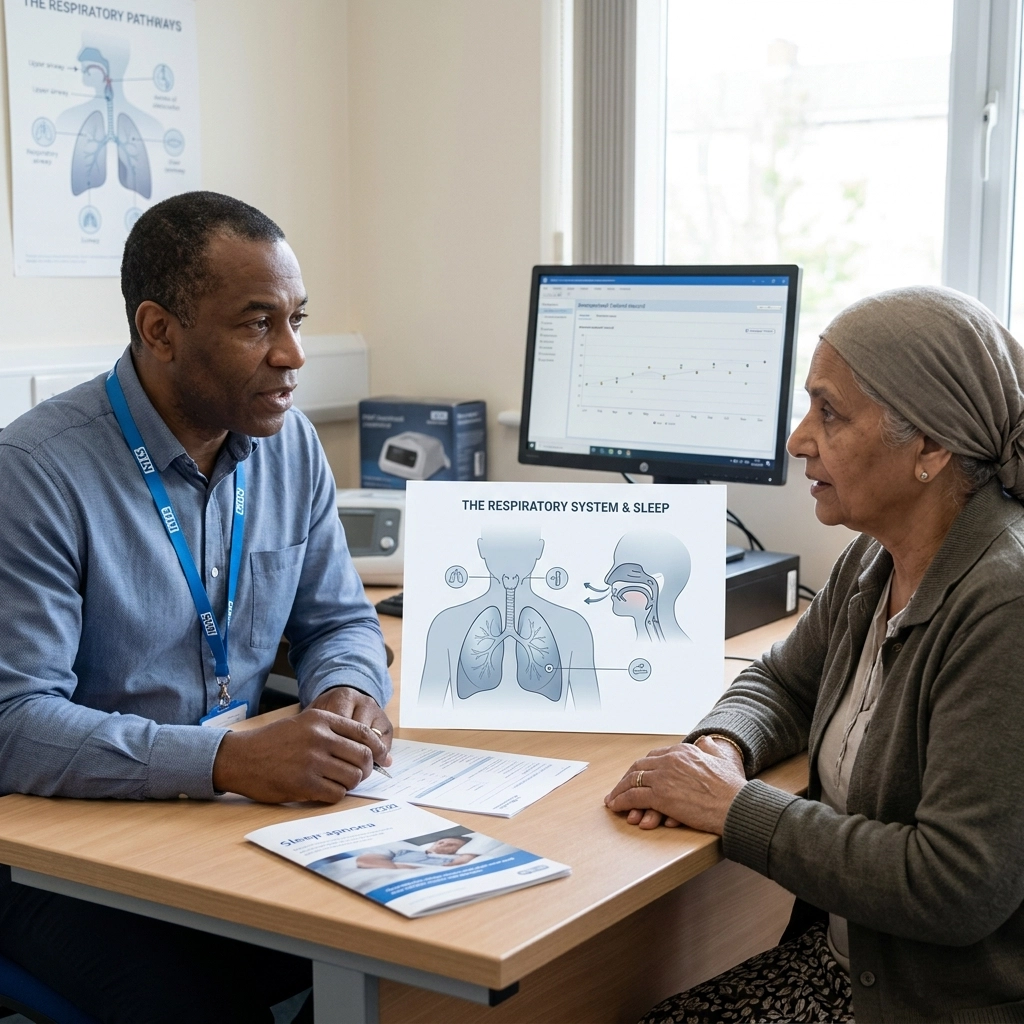
Clinicians often describe how the "reserve" of the lungs is tested during sleep. When the body is horizontal, the mechanics of the chest wall and diaphragm change. For someone with a healthy respiratory system, the body compensates without us ever knowing. However, for those within the respiratory pathway, this transition requires a coordinated effort from both the body and the care team to ensure that the night doesn't become a source of exhaustion rather than recovery.

The Environment: More Than Just a Mattress
What patients and clinicians often describe is that the bedroom environment is a primary stakeholder in respiratory health. We spend roughly a third of our lives in this one room, making it perhaps the most important "clinical" space outside of a hospital.
Air quality isn't just an outdoor issue involving traffic and industry. Indoors, factors like humidity, dust, and temperature can significantly impact how easy it is to breathe overnight. In the UK, where housing stock varies wildly, issues like dampness or poor ventilation aren't just aesthetic problems: they are respiratory ones. When we look at the tag/air-quality, we must consider the micro-climates we create in our own homes.
Simple factors, such as the age of a pillow or the presence of a pet in the room, can change the load on the lungs. It isn’t about being "perfect" or creating a sterile lab; it’s about understanding that the environment is a tool. When Life Sciences and MedTech innovators look at the future of care, they are increasingly looking at how we can monitor and improve these home environments without making them feel like a ward.
Why Sleep is a Multidisciplinary "Team Sport"
There is rarely a perfect dividing line between pulmonology, sleep medicine, and neurology. If a patient is struggling to breathe at night, is it a lung issue? A throat issue? A brain-signal issue? Or perhaps an anxiety-driven issue?
This is why we advocate for a "team effort." A successful journey through the respiratory pathway usually involves a variety of experts working in tandem. This might include:
- Respiratory Physicians: Looking at the primary lung function.
- Sleep Specialists: Analysing the cycles and architecture of rest.
- Physiotherapists: Helping with positioning and clearing airways.
- Primary Care and PCNs: Identifying the early signs of sleep-disordered breathing.
- The Patient and their Family: Providing the lived experience that data alone cannot capture.
In practice, when these groups don't talk to each other, the patient is left navigating a fragmented system while already being exhausted. People often describe how much better things get when a consultant and a community nurse are on the same page regarding a patient's nocturnal care.
The "Brain Fog" and the Lived Experience
One of the most significant impacts of poor respiratory-related sleep is one that doesn't always show up on a lung function test: the "brain fog." When the lungs have to work overtime during the night, the brain doesn't get the oxygen or the deep rest cycles it needs.
Patients often describe a feeling of being "unplugged" the next day. This fatigue affects everything: from the ability to manage their own care to their mental health. It’s a cycle where poor breathing leads to poor sleep, which leads to lower energy to perform breathing exercises or stay active, which in turn leads to worse respiratory health.
Breaking this cycle requires more than just a device or a prescription; it requires understanding the person behind the symptoms. It’s about asking, "How are you feeling at 10 AM?" not just "What is your oxygen saturation?"
Innovation and the Digital Connection
We are seeing a fascinating shift in how we monitor sleep within the NHS. Digital health tools and wearable tech are beginning to bridge the gap between the clinic and the bedroom. Instead of a patient having to spend a night in a sleep lab: which, let’s be honest, is rarely a "normal" night’s sleep: we are moving toward a world where data can be gathered in the comfort of one's own home.
This isn't about surveillance; it's about insight. If a clinical lead can see a trend of declining sleep quality over a week, they can intervene before a full exacerbation occurs. This is the kind of proactive care we will be discussing at our upcoming Round Table 2026 event.

Joining the Conversation
On June 24th, we will be focusing on how we can make these connections stronger. Whether you are a Life Sciences director looking at the next generation of diagnostic tools, an NHS leader trying to streamline the pathway, or someone with lived experience of a chronic condition, your voice is essential.
Respiratory health doesn't stop when we close our eyes. If anything, that is when the most important work of recovery happens. By treating sleep as a collaborative effort: balancing environment, clinical expertise, and technology: we can ensure that "rest" actually means rest.
How to Get Involved
If this is a topic that resonates with you, or if you have insights from your own practice or life, there are several ways to engage with The Respiratory Network:
- The Round Table: Join us for our upcoming event at The King’s Fund on June 24th, where we will be shaping these future conversations: Round Table 2026.
- Stay Connected: Follow The Respiratory Network for future updates and ongoing conversation across the respiratory pathway.
Resting well is a team effort. Let’s make sure no one has to do it alone.
Category: Pathway Excellence
Tags: Respiratory Health UK; NHS Respiratory Services; Lived Experience; Healthcare Networking UK; Patient Engagement UK; COPD; Asthma; Digital Health; NHS Leadership.



Responses